Will reformed human services markets be a good thing for older Australians?
Speech
Commissioner Stephen King gave a speech to the COTA National Forum on 28 June 2018 in Canberra.
Download the speech
Read the speech
Introduction
The first line of the Productivity Commission’s 2011 Inquiry Report on Caring for older Australians states:
Older Australians generally want to remain independent and in control of how and where they live; to stay connected and relevant to their families and communities; and be able to exercise some measure of choice over their care.1
The Commission’s 2017 Human Services Report notes that:
...informed choice can improve outcomes for users because it: empowers people to have greater choice over their lives; enables people to make decisions that best meet their needs and preferences; [and] generates incentives for providers to be more responsive to users’ needs and drives innovation and efficiencies in service delivery.2
Reforms to human services, need to focus on choice. Choice is empowering. Choice gives control to service users — to be able to say what they would and would not like. Choice provides both dignity and respect.
Reforms to human services markets are reforms about choice — and that will be a very good thing for many older Australians.
Alternative approaches to delivering human services
Let me explain.
Broadly, there are two approaches to the delivery of human services. The first is a provider-centred approach. Under this approach service users get told what they can receive, when they can receive it, and who will provide it. They get little if any choice. The funding follows the provider and the service user is disempowered.
Sometimes this provider centred approach will be the best way to deliver a service simply because it is the only effective way to deliver the service. One example is where a service user is not in a position to make a considered choice, such as in an emergency medical situation. But in many situations where we see provider-centred human services today — such as a range of public health services, public housing, and areas of end-of-life care — reforms to improve choice and empower service users are feasible.
The alternative to a provider-centred approach is a user-centred approach where the funding follows the service user, and, in that sense, service users control the funding. With that control, they can choose what services they want to receive, when and from whom. Service users have choice. That choice occurs in a market where alternative suppliers present their case to prospective clients and the clients exercise choice. The choice is not limitless. Government controls both funding and the range of services by the amount of resources they provide service users, through rules of co-payments, by setting minimum standards for service providers and, in some cases, by controlling prices. But, service users are empowered to choose services that best meet their needs and providers have the incentives to develop those services.
What do we mean by ‘reform’ in human services markets?
In reality, many human services are provided somewhere along the spectrum between these two approaches. They have provider-centred elements mixed in with elements of user choice. We see these different mixes, for example, in home-based aged care services in Australia.
Reform in human services markets is often about moving along this spectrum. It is about shifting the provision of human services towards a ‘user choice’ approach. It is about changing the way services are provided so that the focus is on the service recipient rather than the service provider.
So, will reforms to human services markets to improve choice be a good thing for older Australians? Yes — so long as they are designed appropriately.
How do we reform human services markets?
Market-based competition
First, we need market-based competition. Choice can only be effectively exercised if there are alternative providers offering alternative services.
So effective market reform for human services needs workable competition between service providers. For choice to be feasible there needs to be multiple providers offering services that all meet minimum standards but are also differentiated – bespoke services that can best meet different users’ needs.
It is sometimes argued that competition is not needed for choice; that one provider offering multiple services will do. This is wrong.
Having one designated provider who supplies a list of alternative options is not effective choice. The service user will be at the mercy of the monopoly provider. And the monopoly provider has no incentive to innovate and better meet users’ needs.
Similarly, having multiple providers who offer the same service that is tightly designated by the government is not meaningful choice. It is like ‘pick a box’ where each box holds the same prize.
Workable competition between service providers is the key to meaningful choice for service users. But in some situations, such competition may not be practical. For example, in some rural and remote areas there may be few, if any, potential service providers. The Productivity Commission recognised these practical constraints in its Human Services Report.3
Information and guidance
Second, service users need access to and help with information. Service users cannot make appropriate choices without relevant information. Sometimes service users will need navigators — someone who can provide guidance and help them choose services that best suit their needs. Appropriate market reforms in human services do not assume that service users can simply ‘work it out’.
For example, when considering reforms to public hospital services, the Productivity Commission noted the need for patients to have better information — like that available in England under their National Health Service. But we also saw the role of GPs to help patients navigate that information.4
Recipients of human services in Australia often operate in either an information vacuum or suffer information overload. There is either little information — for example about the performance of or even the fees charged by our medical specialists — or reams of often complex information that confuses — such as in some areas of aged care services.
Effective market reform for human services require reforms to information and guidance. Service users require clear information with access to navigators where needed.
Careful reform design
Third, reforms to human services need to be carefully designed. Human services markets are not like many other markets. For example, the service user may be paying none of, or only some of the price. Governments foot much of the bill, reducing the incentives for service users to make sure they receive value for money. The services are often complex and current decisions have long term consequences for service users. And in some situations, the party making the choice is not the service user but an agent acting on their behalf.
These features mean reforms in human services need careful design and testing, to ensure that they make service users better off. Poor reforms — whether focused on choice and markets or on a provider-centred approach — can harm, not help, service users. The Productivity Commission has referred to this as the need for effective government stewardship.5
We have seen some poorly designed reforms. For example, the use of crude performance indicators on waiting times in public hospitals has led to poor outcomes for patients, both here and overseas.6
Carefully designed reforms build protections for service users. For example, the NDIS Quality and Safeguards Commission is part of the National Disability Insurance Scheme. It aims to 'support NDIS participants to exercise choice and control, ensure appropriate safeguards are in place for NDIS supports, and establish expectations for providers and their staff to deliver quality support'.7
Similarly, the recent jailing of a man with mental health problems highlighted the importance of both a 'default' service provider where individuals are unable or unwilling to choose, and a 'provider of last resort' where service providers are generally unable or unwilling to meet a service user's needs.8
All reforms need careful design. But this is not a reason to either avoid reforms that can improve outcomes for service users or to ignore current system failings.
Transition
Finally, all reform, by definition, requires transition. This transition needs to be carefully planned, allowing for testing and trialling; timeframes that are long enough for users and providers to adjust, without unnecessarily delaying the benefits of reforms to users; and flexibility so that adjustments can occur to the transition path in real time.
Designing and managing transition is hard.
The Productivity Commission has recently completed a Study Report on the National Disability Insurance Scheme (NDIS) Costs. That report noted the 'unique and challenging' nature of the transition period as the NDIS reforms are rolled out.9
It also noted that the initial 'rollout timetable for participant intake will not be met'.10
Potential problems in transition are rarely a reason to avoid reform. And in Australia, we are in the fortunate situation that further reforms to human services can benefit from experience learnt, both here and overseas, from past reforms.
Conclusion
Will reformed human services markets be a good thing for older Australians?
In general, yes.
Indeed, they will be a good thing for many Australians.
Moving human services down the spectrum, away from provider-centred approaches and towards user choice in carefully designed markets, can provide many benefits. There are risks — but these are decreasing with experience. And the rewards, for the service users, their families, and the broader community, can be great.
Footnotes
- Productivity Commission 2011, Caring for older Australians, Inquiry Report No. 53, 28 June, Canberra at p.xix. Return to Footnote 1 in the text
- Productivity Commission 2017, Introducing competition and informed user choice into human services: Reforms to human services, Inquiry Report No. 85, 27 October, Canberra at p.5. Return to Footnote 2 in the text
- For example, when considering public dental services (op. cit. note 2, recommendation 13.5).Return to Footnote 3 in the text
- Op. Cit. note 2 at Chapter 10. Return to Footnote 4 in the text
- Op. Cit. note 2 at Chapter 2. Return to Footnote 5 in the text
- Op. Cit. note 2 at Box 2.5. See also Nocera, A. 2010 'Performance-based hospital funding: a reform tool or an incentive for fraud?' The Medical Journal of Australia, 192(4), 222-224. Return to Footnote 6 in the text
- See https://www.dss.gov.au/disability-and-carers/programs-services/for-people-with-disability/ndis-quality-and-safeguards-commission (accessed June 27, 2018). Return to Footnote 7 in the text
- For example, see Younger, E. 2017, 'Man with intellectual disability released from Melbourne prison after judge ‘horrified’ by conditions' ABC news, www.abc.net.au, November 24 (accessed June 27, 2018). Return to Footnote 8 in the text
- Productivity Commission 2017, National Disability Insurance Scheme (NDIS) Costs, Study Report, October, Canberra p.10. Return to Footnote 9 in the text
- Op. Cit note 9 at p.12. Return to Footnote 10 in the text
Speech
Chair Danielle Wood presented to the National Conference on University Governance.
Download the speech
Read the speech
Thank you everyone for the opportunity to speak tonight. I am honoured to stand on the land of the Wurundjeri people of the Kulin Nation and I pay my respect their elders past and present. I extend that respect to any Aboriginal and Torres Strait Islander people in the audience today.
I’m sure it’s something of a cruel and unusual punishment making you sit through a speech on productivity before you get your dessert. I hope I can convince you that productivity is its own treat, and a substantial one at that. As the Nobel Prize winning economist Robert Lucas said: ‘Once one starts to think about [economic growth], it is hard to think about anything else.’ 1
But beyond (hopefully) convincing you that productivity matters, I want to focus on the unique role of universities as engines of productivity. And I will issue a challenge: for universities to step up their own productivity performance so as to deliver more of the research and quality teaching Australia needs for us to thrive in coming decades.
Productivity – why do we care?
Productivity is about improving our living standards. If we can produce more goods and services using the same or fewer resources than before, that’s productivity growth.
And the effects of that growth over time are enormous.
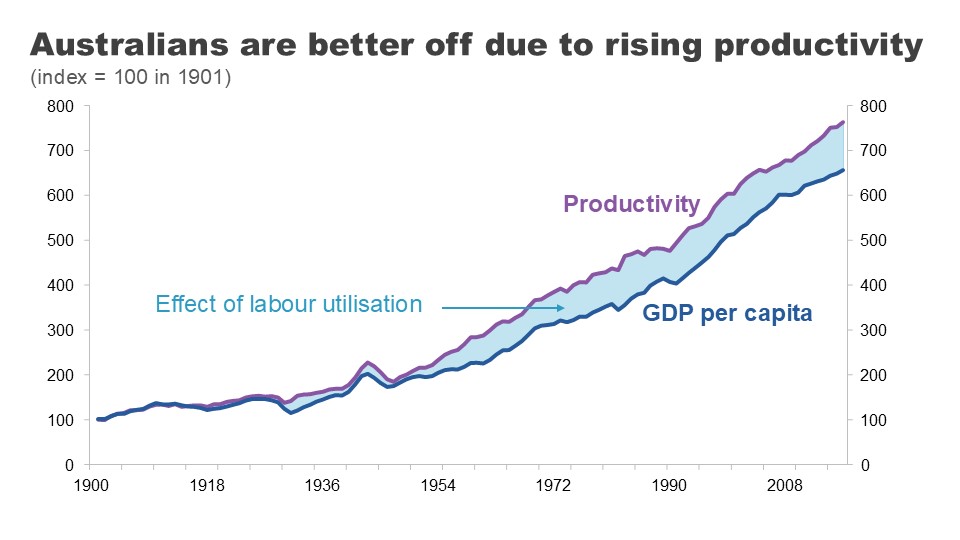
In 1901 in Australia, it took 18 minutes of the average worker’s time to afford a standard loaf of bread. Today, it is just 4 minutes.’ 2
The productivity of our bread makers means that we can all consume a lot more bread – or for the carb conscious – spend that extra bread money elsewhere.
But it’s not just bread production that’s been revolutionised.
A theatre ticket cost an average worker 321 minutes of work in 1901. Today it’s 62. A bicycle? 473 hours in 1901 down to just 6 hours today.
And to put even today’s very real concerns about rental costs into perspective: the typical Australian worked 9 hours a week to afford a rental in 2019 but 20 hours in 1901.
Wherever you look, productivity progress has improved our capacity to deliver the goods and services that we value.
That productivity growth has seen real per person incomes improve by more than 700% since Federation, while giving us an extra 13 hours a week to ourselves.’ 3
But here let me engage with a common argument dismissing the importance of productivity. According to the doubters, this economic growth might deliver more ‘stuff’ but does not deliver better lives or improved wellbeing.
I would mostly disagree. It is certainly true that economic growth won’t tuck your kids into bed at night, but it has delivered at lot more than just extra bread or bicycles.
Growth is correlated with so many of the things we care about: longer, healthier lives, better education, more and more varied leisure time, and better and more stable political institutions.
Many of these things are supported by growth but they also support growth themselves. As I’ll explain shortly, this is very much the case with education.’ 4
That’s why it’s not surprising that richer countries tend to have higher average life satisfaction’ 5 and that those countries that experience sustained economic growth tend to see their average levels of satisfaction increase over time.’ 6
That said, economists recognise that growth is not a measure of everything we care about. Some things are hard to measure well, like the quality of care services. And important determinants of wellbeing like community involvement and quality of relationships are missed all together.
But no one can or should deny that growth matters.
Houston, we have a (productivity) problem
I don’t need to tell this audience that Australia’s recent productivity performance hasn’t been much cause for celebration.
Productivity went on a roller coaster ride during COVID.
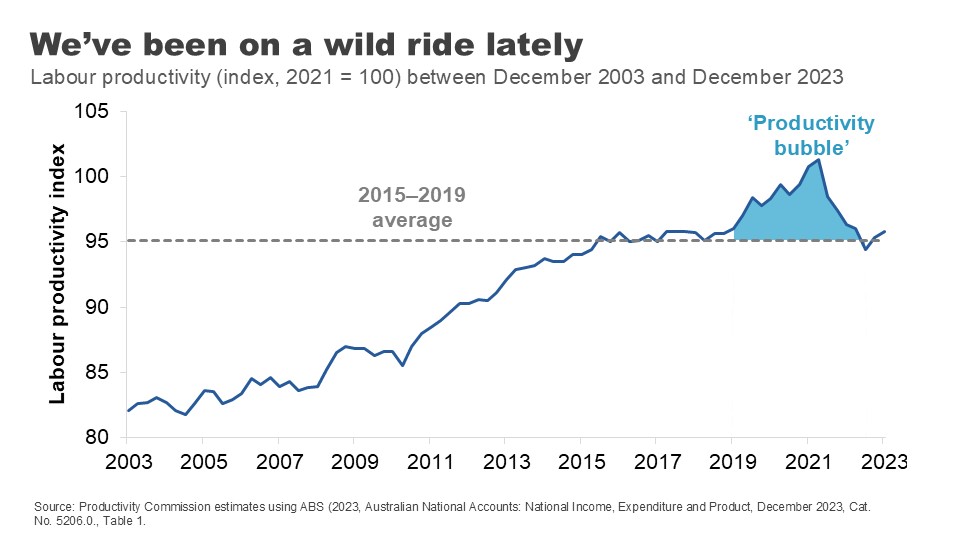
In the first two years of the pandemic, productivity rose strongly. This counterintuitive result was primarily because social distancing restrictions reduced hours worked the most in the lower-productivity services sectors.
But this productivity ‘bubble’ was in no way sustainable. After the end of restrictions in 2022, working hours expanded again in these sectors and pushed productivity in the opposite direction. The bubble burst.
The strong performance of the labour market through much of 2022 and 2023 has also put downward pressure on productivity during this period.
Now let me be totally clear: strong labour markets are great. But the surge in hours worked in the COVID recovery (coming from increased participation, lower unemployment and the re-opening of borders) was both quick and large. The capital stock has not kept up. The historical decline in the amount of capital per worker, has dragged on productivity because each worker has less capital – fewer or less efficient tools and resources – to help them do their jobs.’ 7
In some ways, the economy is like the cobra swallowing the ‘rat’ of the COVID shock. It will digest it, but it will take some time.
But this begs the question: what is the economy recovering to?
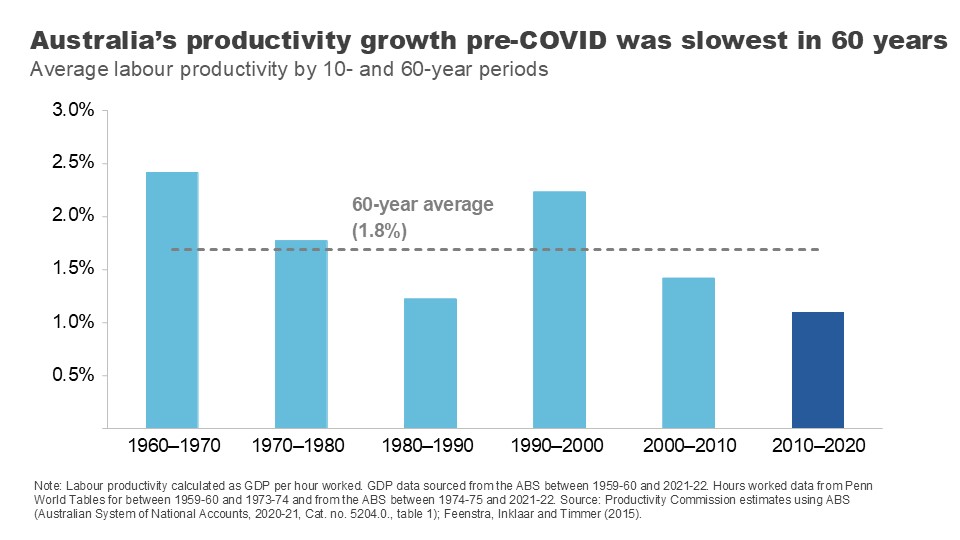
Even before our COVID rollercoaster, all was not well.
In the decade sandwiched between the GFC and COVID, Australia’s annual productivity growth averaged just 1.1% – the lowest of the last 6 decades and well below its 60-year average.
This slowdown in productivity growth is not just an Australian phenomenon.
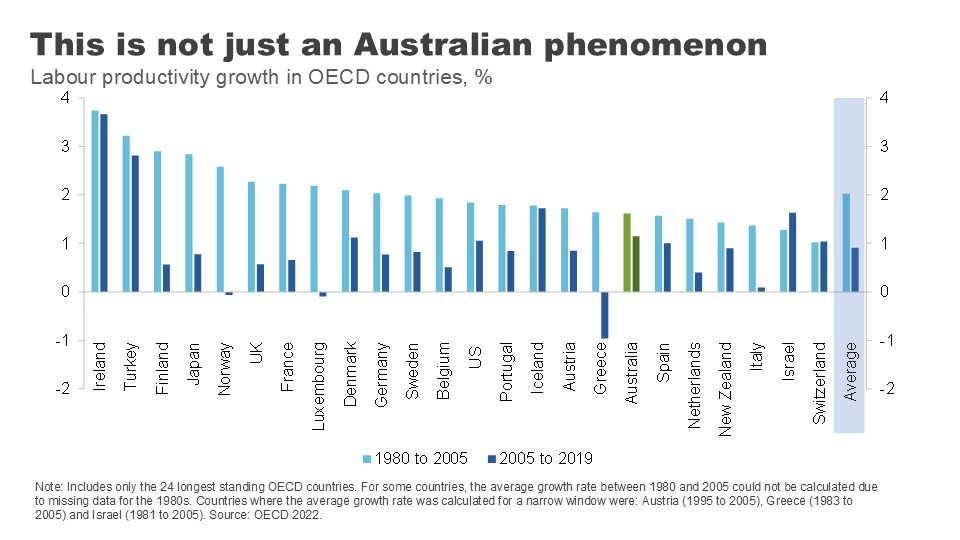
Almost every OECD country experienced a substantial decline in labour productivity in the 15 years prior to COVID, compared to the previous 15. Across the OECD, labour productivity growth halved in this period.
A range of credible explanations have been put forward to explain why: growth in the lower productivity services sector, declining gains from education, a smaller contribution from technological change, reduced economic dynamism, and increased risk aversion by business and capital owners.
But what I want to focus on here are two that are most relevant to our universities: declining gains from education and declining contribution from innovation. And then I want to address how the people in this room can help turn them around.
Universities are a powerful engine for productivity
Universities contribute a huge amount to our intellectual, social and cultural lives. But you’ve an invited an economist tonight so I’m naturally going to talk about the ways in which universities contribute to our long-term productivity performance.
There are, I think, three major channels:
- through building the skills and capacity of our future workforce – the so called ‘human capital’ of our population
- by generating and disseminating the research and ideas that lead to better processes and new and improved goods and services, and
- through building ties, understanding and goodwill with people from other nations, which contributes to ongoing integration – whether through trade, investment or the flow of ideas.
Tonight, I’m going to focus on the first two.
Boosting human capital
Let me start with the fundamental role that universities play in educating the population.
In the past 30 years, education levels across the Australian population have soared.
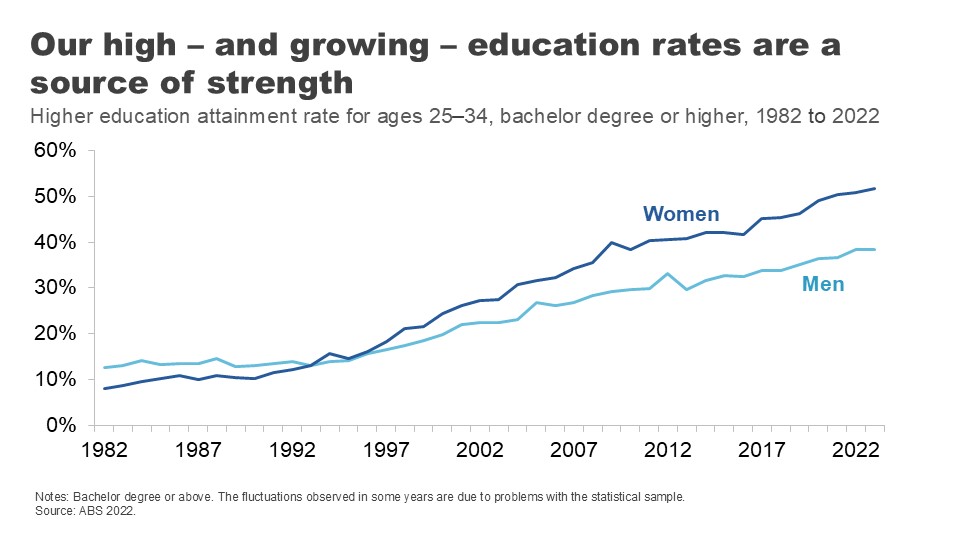
In the early 1980s, about one in ten 25–34-year-olds had a held a university qualification. Today, it’s 45%.’ 8
Part of this increase has been driven by a strong migration program that has encouraged skilled migrants to settle on our shores.’ 9 But it points as well to a large and sustained expansion in the number of Australians going to university.
Annual domestic student course completions have more than doubled since 1989, with nearly 140,000 students finishing a bachelor’s degree in 2021 and 87,000 finishing post-graduate study.’ 10
The resultant improvement in ‘labour quality’ has played an important role in productivity growth – particularly as other contributors have stalled.
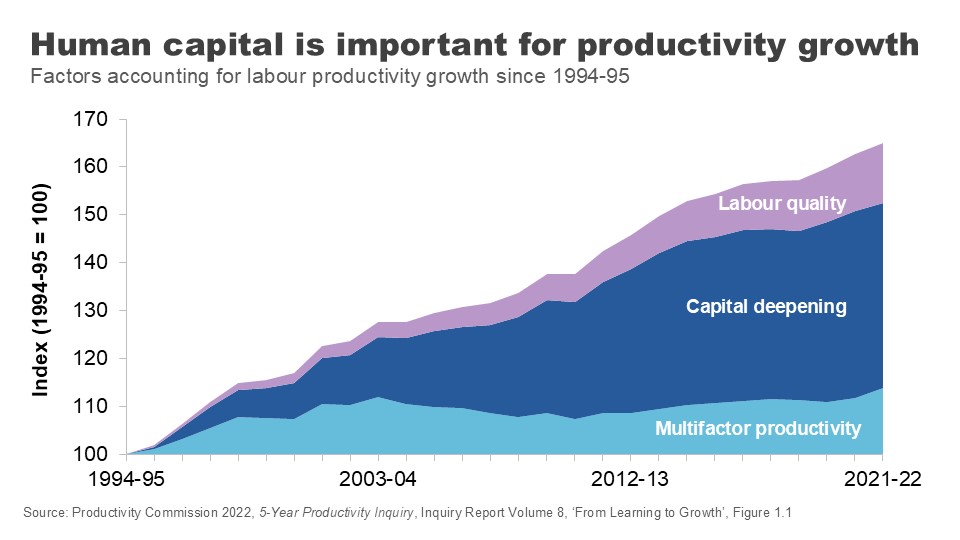
University degrees are associated with better employment outcomes and higher earnings over people’s lifetimes – even after adjusting for individuals’ characteristics.’ 11
Although the graduate premium is in decline,’ 12 it is still significant across the lifetime.
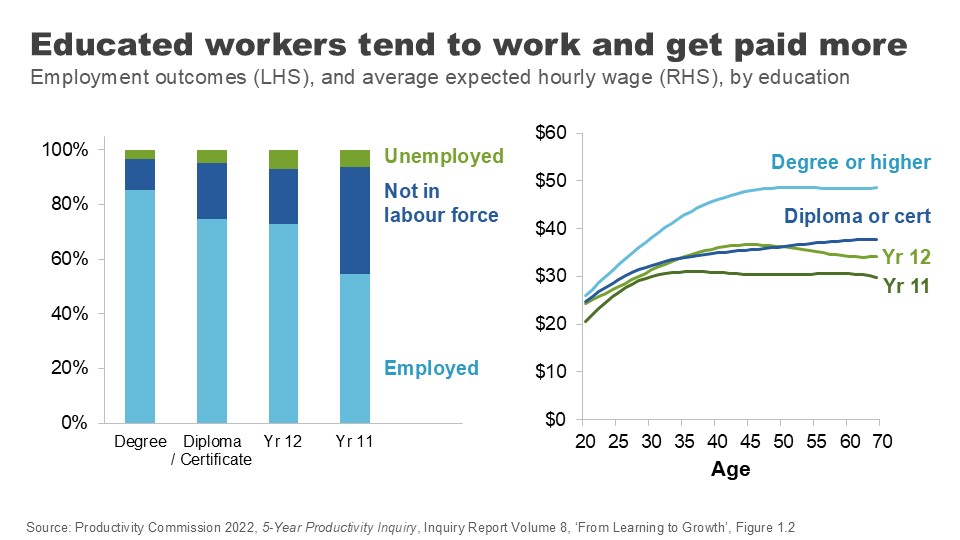
Higher levels of education in our working population improves wages and productivity through a few channels.
Most obviously, it improves the skills and abilities of our future workforce.
People who hold a tertiary qualification have higher cognitive performance than others their own age, even when you control for the fact that clever people tend to go on to study at higher levels. 13
Perhaps just as importantly, people with a higher education are more likely to do on-the-job training when they’re in the workforce – they’ve learned how to learn. 14 And there’s evidence going to university improves your non-cognitive skills, like sociability and your ability to cooperate or work in a team. 15
Education also improves people’s capacity to innovate. Increases in the supply of educated workers and managers leads to greater direct innovation by firms. Those educated workers are also more likely to adopt new innovations from elsewhere. 16
This link between education and an innovation mindset is critical if we are to supercharge the productivity upside from education, a point I will return to.
There are still gains to be eked out from expanding Australians’ access to higher education, despite the huge expansion over recent decades.
As the Productivity Commission noted in our 2023 Productivity inquiry, there is no evidence that we have reached the point where the cost of education for marginal workers outweighs the benefit received by them and by society. 17
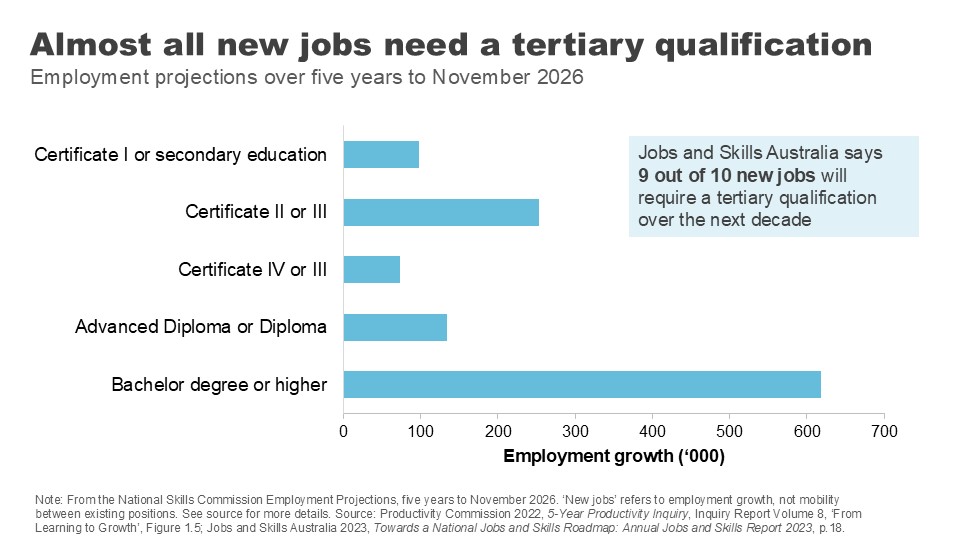
According to Jobs and Skills Australia, more than 9 out of 10 new jobs will require a post-school qualification over the next decade, and around 50% will require a bachelor's degree. 18
The recent Universities Accord argued governments should continue to promote participation in university and vocational education and set ambitious targets for governments to boost attainment rates by 2050.
The benefits of higher education are why the PC has supported a return to a system of uncapped demand driven funding. 19
But even with this potential upside, the huge ramp up in the education levels of the population will not be repeated. This means the contribution of gains from the quantity of education in the productivity numbers is likely to be more subdued in coming decades than in the previous ones.
This brings the quality of education into even sharper focus.
Education quality: levelling up
Improving education quality means improving outcomes for students for a given level of investment.
Which begs the question: how are we currently faring?
As already mentioned, university graduates have good labour market outcomes over the medium term compared with those who acquire skills via VET or school alone, even after adjusting for student characteristics.
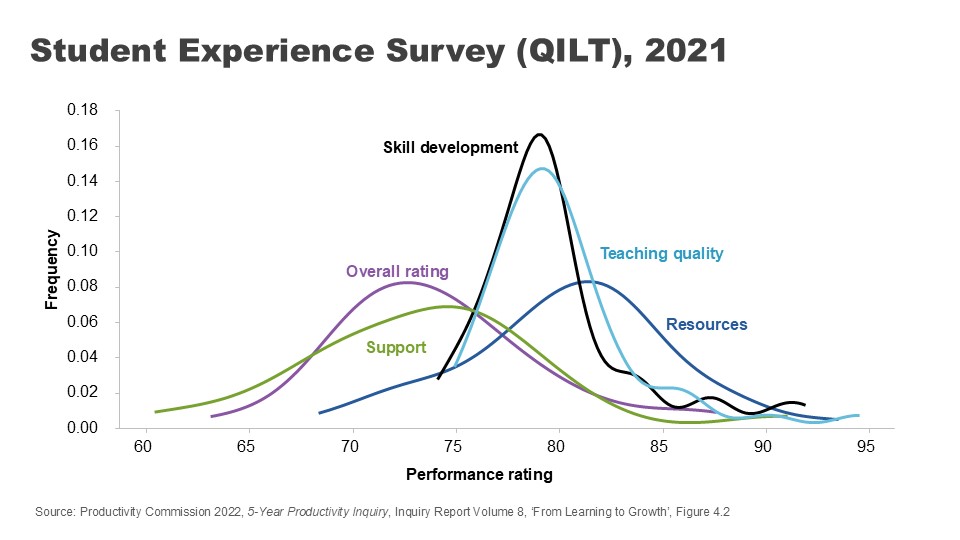
Australian universities also perform well overall on student-assessed measures of quality. Indeed, the average university brings home a 76% – just scraping through with a distinction – on overall experience for undergraduate students. 20 On assessed teaching quality, it’s 80% – a solid mark. 21
Further, on measures of employer satisfaction, overall satisfaction with graduates sits just below 84% and has remained strong over time. 22
But there are reasons to be vigilant.
Despite the relatively strong average student-assessed quality scores, there is a fair degree of variation across institutions.
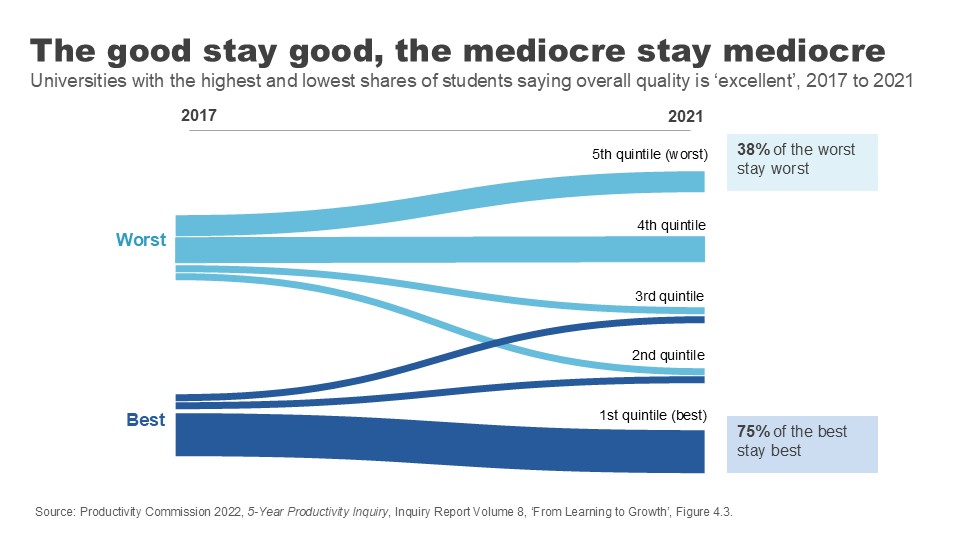
There is also stickiness in the outcomes data, suggesting a lack of course correction. Measured over a 4-year period, the universities that start with the highest share of students nominating their quality as ‘excellent’ tend to stay excellent, while those with the lowest shares also tend to stay at the bottom.
Employer satisfaction scores, while high overall, are stronger for foundational and technical skills than broader job skills like collaboration and adaptation. 23
And employers report much lower levels of satisfaction with the collaboration skills of graduates who study entirely remotely. 24 This matters because these ‘social skills’ are increasingly demanded by employers as a complement to technical skills. 25
More generally we need to consider the impact of online course delivery for student learning. The shift to online adds convenience and flexibility for students, but it comes with risk to quality.
Measures of learning engagement dropped when the pandemic hit our shores, and have not recovered since. 26
We may have jumped many of the initial hurdles to hybrid learning during those chaotic months of shutdowns, but not everyone has yet nailed the challenge of how to do online delivery well. A sea of blank Zoom screens is not ideal for either students or teachers.
More broadly, the Productivity Commission has noted the lack of direct incentive for teachers and universities to improve teacher quality.
We’re used to looking at star ratings when we book a hotel or a restaurant, but prospective students often don’t have good data when choosing between courses. 27
This lack of visibility combines with other factors – a general sense that teaching hold less prestige than research, government funding settings that fail to reward quality, and a lack of external oversight – to weaken the incentives for delivering the best teaching. 28
Of course, there are non-pecuniary incentives for individuals and institutions to teach well. And indeed, intrinsic motivations for excellence continue to steward high quality and innovative teaching practices at our universities.
But that is not enough to ensure that every teacher is delivering at a high standard.
The PC has put forward a range of recommendations for change. An important one is making lecture and course materials publicly available. Letting the public see behind your high walls would sharpen the incentives for quality teaching, allow students to make better decisions around what courses might match their interests and assist in lifetime learning – giving those not looking for an accreditation access to an endless supply of learning opportunities. 29
We need to ensure that teaching excellence is at the heart of our universities if we are going sustain the big improvements in quality needed for future productivity gains.
Promoting innovation
I want to turn now to another critical way in which universities impact our prosperity – in their role as vectors for innovation.
It is technological change that drives most productivity improvements over time. 30 And it is ideas that make technological change possible.
Economics Professor Daniel Susskind has argued that asking ‘how do we generate more growth?’ is essentially the same as asking ‘how do we generate more ideas?’.
And what are universities if not factories for ideas? 31
It is worth remembering that when we talk about ideas we are not just talking about the novel, frontier research that some of your researchers might be engaged in. ‘New to the world innovation’ is only around 1-2% of Australia’s innovation story. Diffusion – the application of existing knowledge to different businesses and contexts – is a crucial part of the innovation puzzle. 32
‘Innovation for the 98%’ must also be a focus of research efforts and graduate skills sets.
Universities spend more than they used to on research activity. Total university research expenditure has increased five-fold since the early 1990s – although growth has slowed somewhat in recent years.
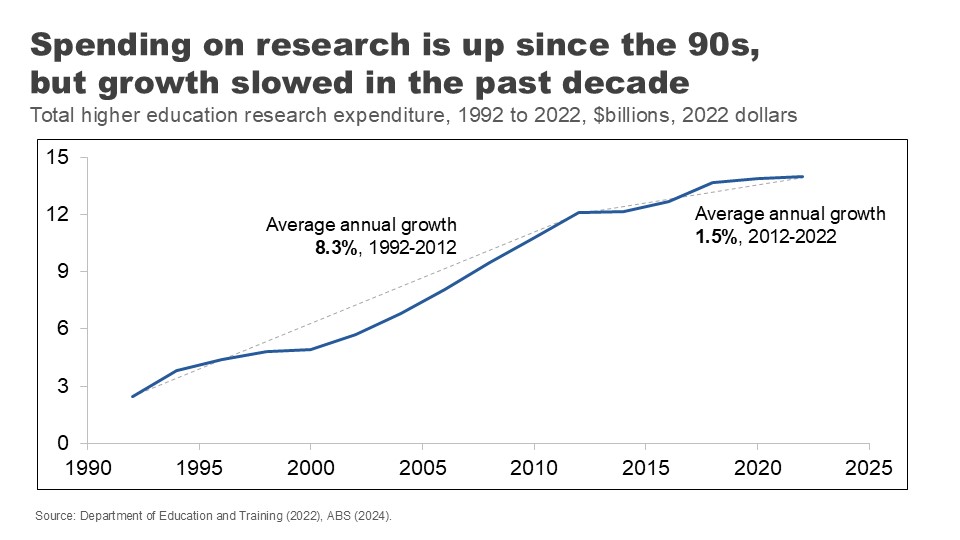
This ramp up in spending over the past three decades is repeated across much of the developed world. But it has not generated the ideas boom we might have hoped.
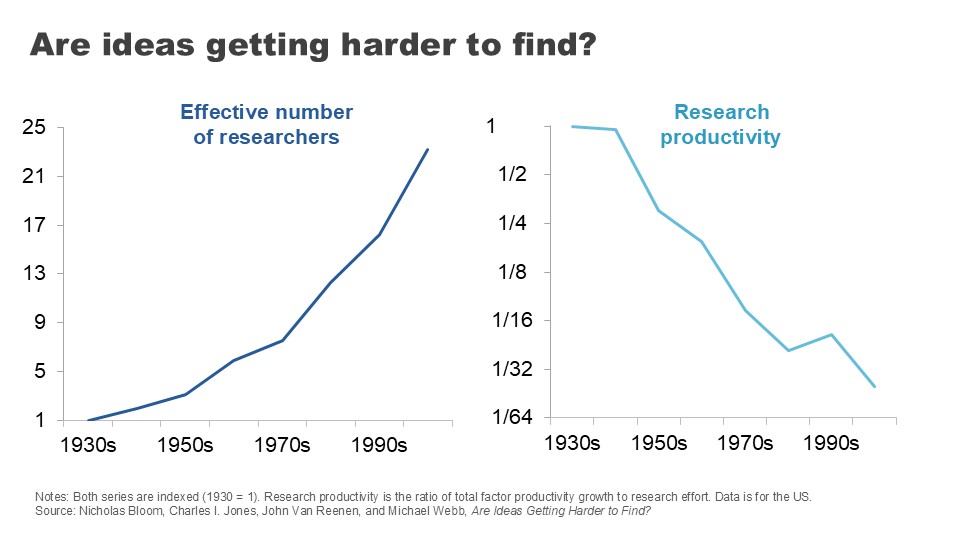
For example, if we turn to the US, we can see the number of people employed in research roles has grown 23-fold since the 1930s – a huge expansion in research effort. 33
But measured by the economic outputs of this research – the expansion in total factor productivity across the economy – the productivity of that research has declined 41-fold – or a growth rate of minus 5.1% per year on average. 34
This tale of more and more effort and for less and less return has played out across a range of innovation areas.
Take Moore’s Law: the tendency for the number of transistors fitted onto an integrated circuit to double every two years. It is, on the face of it, a remarkable testament to our capacity for innovation. But the number of researchers required to bring about this result has grown to be 18 times higher than it was in 1971. 35
Agricultural crop yields are improving at a relatively constant or slightly declining rate, but the number of agricultural researchers required to achieve this has doubled. 36
In drug discovery, the number of new drugs approved per billion on R&D halves every nine years or so, in a phenomenon that has been dubbed ‘Eroom’s Law’: Moore’s law spelled backwards. 37
At the heart of the slowdown in research productivity is that researchers inevitably solve the easier problems first – making gains harder once the lowest hanging fruit has been picked. Indeed, being ‘Better than the Beatles’ is a challenge that confounds across so many research areas. 38
But even noting this difficulty, there is still scope to improve the productivity of the research process in ways that could help generate and diffuse new ideas.
Australia is unusual in that university-led research makes up a relatively large percentage of our R&D expenditure. 39
As a share of GDP, our universities chip in more for research and development than universities in the US and Korea, and we’re well above the OECD average. 40
The good news is that our university research is top notch on academic metrics.
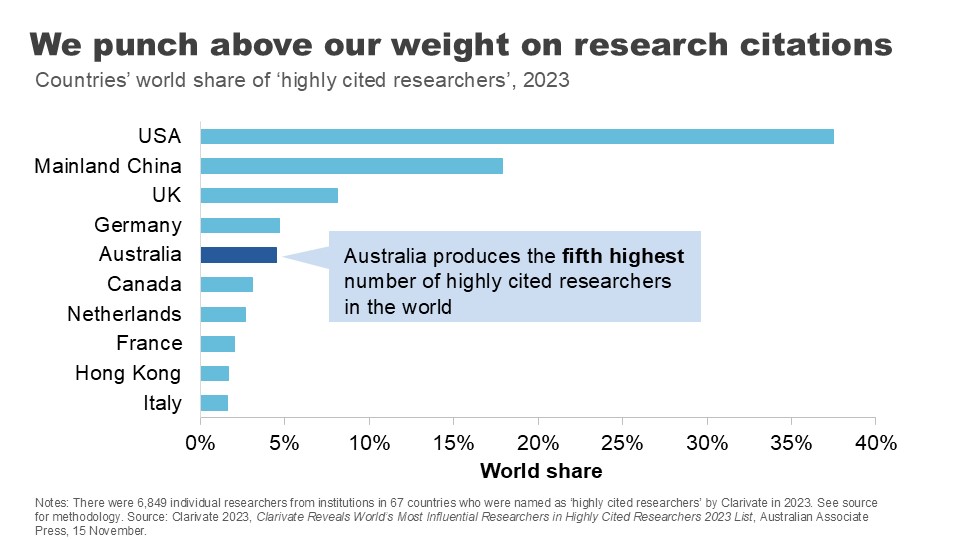
Despite our small population, we have the fifth highest number of highly citied researchers in the world. 41 And 84% of our research is rated at or above world standard. 42
Australian researchers also are more likely than those in the US or the EU to collaborate with international scholars, allowing us to ‘hoover up’ good ideas from overseas and apply them at home. 43
But there’s more we need to do.
There is a widely held view that Australian business collaboration with universities is poor. The perception is backed up in the numbers: data from the ABS suggests less than 10% of innovating firms got their ideas from universities between 2019 and 2021. 44
As much as policy makers say they want universities and business to ‘talk more’, clearly the incentives aren’t there to bring everyone to the table.
The Accord recognised the importance of nationally-relevant research in its recommendation for a new ‘Solving Australian Challenges Fund’ which would reward universities that apply their research capabilities to meeting Australia’s ‘big national challenges’. 45
Even where research turns up potentially useful ideas for Australian businesses or policy makers, we could do more to put them into practice.
Governments have long grappled with reducing barriers to research commercialisation – such as IP licencing and academic-spin offs or joint ventures – only partially successfully.
But the PC’s found we should be doing more to encourage knowledge transfers by encouraging labour mobility between industry and academia, and even by promoting joint conferences and networking events.
We can also help businesses tap into the experience and knowledge of academic researchers by reducing barriers to academic consulting, which is too often held up by administrative roadblocks. 46
There is also more to do on the productivity of the ideas generation process itself.
Long and expensive processes for grants can reduce ‘bang for buck’ and slow the research process.
US research on the peer-reviewed grant-making process concluded that the ‘tax’ of application processes may be up to 45% of researcher time. Further, these processes can skew or bias research efforts in a number of ways: towards more incremental research with a higher likelihood of surviving review than riskier or novel research; against interdisciplinary research; and towards researchers with a history of successful applications. 47
Certainly it does not take long for a conversation with Australian academics to degenerate into a similar set of complaints.
The recent Accord process suggested universities be paid for the indirect costs of applying for nationally competitive research grants, 48 and the Australian Research Council recently took the positive step of introducing an Expression of Interest round to its Discovery grant applications. 49
Future work may be necessary to explore alternative models like ‘science lotteries’ to continue tackling these challenges. 50
Where to from here?
I realise tonight I am speaking to a sector working through significant upheaval.
The COVID shock – the rollercoaster ride of closing and then reopening international borders with flow on effects for international student numbers – was obviously hugely challenging. Universities are on the frontline of a major technological change with the shift to online teaching and the growing adoption of generative AI in both learning and research.
Those challenges have been amplified by big and disruptive policy changes over a short period: first with the Jobs Ready Graduates package, then a suite of regulatory reforms to student migration settings, 51 and now the proposal for international student caps.
The Universities Accord process, a generally more constructive policy exercise, is also starting to flow through to policy. But it has raised fundamental questions about the university business model and the extent to which we can continue to rely on international student revenue to ‘cross subsidise’ research activity.
I am here tonight to say the payoff from getting the policy settings and the internal culture right are high. Universities hold in their hands two crucially important ingredients for national productivity: the skills of our labour force and the generation and diffusion of ideas.
Gains in both of these areas are becoming harder to come by. That might naturally push you to look for more resources. But I’m here to encourage you to also look for improvements via productivity at home.
Promoting teaching excellence, widely sharing learning, supporting research with Australian impacts and empowering students with an innovation mindset are just some of the ways in which Australia’s universities can shape a more productive future for Australia.
Footnotes
- Lucas RE Jr 1988, On the mechanics of economic development, Journal of Monetary Economics, Vol. 22, Issue 1, p.5. Return to text
- Productivity Commission 2023, 5-year Productivity Inquiry: Keys to growth, Vol. 2, Inquiry Report no. 100, Canberra, p. 6. Return to text
- Ibid., p.17. Return to text
- Susskind D 2024, Growth: A Reckoning, Penguin Books, United Kingdom. Return to text
- Sacks, D, Stevenson, B & Wolfers, J 2010, Subjective Well-being, Income, Economic Development and Growth, NBER Working Paper, No. 16441, October. See also Ortiz-Ospina, E. & Roser, M. 2013, Happiness and Life Satisfaction, Our World in Data, https://ourworldindata.org/happiness-and-life-satisfaction, (updated February 2024; accessed October 2024). Return to text
- Ortiz-Ospina, E & Roser, M 2013, Happiness and Life Satisfaction, Our World in Data, https://ourworldindata.org/happiness-and-life-satisfaction, (updated February 2024; accessed October 2024). Return to text
- Productivity Commission 2024, Quarterly Productivity Bulletin – June 2024, 27 June, Canberra. Return to text
- ABS 2023, Education and Work Australia, Table 35. Return to text
- See Norton, A 2023, Mapping Australian Higher Education 2023, ANU Centre for Social Research and Methods, for a discussion. Return to text
- Ibid., p.52. Return to text
- See Productivity Commission 2023, 5-year Productivity Inquiry: From Learning to Growth , Vol. 8, Inquiry Report No. 100, Canberra, pp.4-6, for a discussion of literature and controlling for cofounders. Return to text
- Brennan, M 2022, Productivity, Migration and Skills , ‘Rebuilding Australia’s Future’, Universities Australia Conference, delivered 7 July. Return to text
- Productivity Commission 2023, 5-year Productivity Inquiry: From Learning to Growth , Vol. 8, Inquiry Report No. 100, Canberra, pp.4-6. Return to text
- Ibid. Return to text
- Ibid. Return to text
- Ibid. Return to text
- Ibid, p. 3. Return to text
- Jobs and Skills Australia 2023, Towards a National Jobs and Skills Roadmap: Annual Jobs and Skills Report 2023 , Australian Government, October, p.18. Return to text
- Productivity Commission 2023, 5-year Productivity Inquiry: From Learning to Growth , Vol. 8, Inquiry Report No. 100, Canberra, Recommendation 8.4, p. 64. Return to text
- Quality Indicators for Learning and Teaching (QILT) 2023, 2022 Student Experience Survey , Department of Education, Table 1. Return to text
- Quality Indicators for Learning and Teaching (QILT) 2023, 2022 Student Experience Survey , Department of Education, Figure 1. Return to text
- Quality Indicators for Learning and Teaching (QILT) 2024, 2023 Employer Satisfaction Survey , Department of Education, Figure 1. Return to text
- Ibid., Table 3. Return to text
- Ibid. Return to text
- Brennan, M. 2022, Productivity, Migration and Skills , ‘Rebuilding Australia’s Future’, Universities Australia Conference, delivered 7 July. Return to text
- Quality Indicators for Learning and Teaching (QILT) 2023, 2022 Student Experience Survey , Department of Education, Figure 1. Return to text
- The PC recommended QILT data be refined and made more salient for prospective students. Productivity Commission 2023, 5-year Productivity Inquiry: From Learning to Growth , Vol. 8, Inquiry Report no. 100, Canberra, Recommendation 8.9, p. 111. Return to text
- Ibid., pp. 97-101. Return to text
- Ibid., Recommendation 8.9, p. 111. Return to text
- Williamson et al. 2015, Technology and Australia’s Future: New Technologies and their Role in Australia’s Security, Cultural, Democratic, Social and Economic Systems , Australian Council of Learned Academies. Return to text
- Susskind D 2024, Growth: A Reckoning , Penguin Books, United Kingdom, p.177. Return to text
- Productivity Commission 2023, 5-Year Productivity Inquiry: Innovation for the 98% , Vol. 5, Inquiry Report no. 100, Canberra. Return to text
- Bloom et al. 2020, Are Ideas Getting Harder to Find? , American Economic Review, Vol. 110, No. 4, pp. 1104-1144. Return to text
- Ibid. Return to text
- Ibid. Return to text
- Ibid. Return to text
- Scannell et al. 2012, Diagnosing the Decline in Pharmaceutical R&D Efficiency , Nature Reviews Drug Discovery, Vol. 11, No. 3, pp. 191-200. Return to text
- Ibid. Return to text
- O’Kane, M. et al. 2024, Universities Accord: Final Report, Australian Government, Figures 30 and 31. Return to text
- Ibid. Return to text
- Ibid, p.192. Return to text
- Ibid. Return to text
- Ibid. Return to text
- Productivity Commission 2023, 5-year Productivity Inquiry: From Learning to Growth , Vol. 8, Inquiry Report no. 100, p.49. Return to text
- O’Kane, M. et al. 2024, Universities Accord: Final Report, Australian Government, p. 299 Return to text
- Productivity Commission 2023, 5-Year Productivity Inquiry: Innovation for the 98% , Vol. 5, Inquiry Report no. 100, Canberra, Recommendation 5.4, pp. 50-52. Return to text
- See Sharma, I. et al. 2022, Piloting and Evaluating NSF Science Lottery Grants: A Roadmap to Improving Research Funding Efficiencies and Proposal Diversity , Institute for Progress, 2 February, for a summary. Return to text
- O’Kane, M et al. 2024, Universities Accord: Final Report, Australian Government, p. 216-217. Return to text
- Australian Research Council 2023, Discovery Projects Scheme: Two-stage Application Process , 30 October, https://www.arc.gov.au/news-publications/media/feature-articles/discovery-projects-scheme-two-stage-application-process (accessed October 2024). Return to text
- Sharma, I et al. 2022, Piloting and Evaluating NSF Science Lottery Grants: A Roadmap to Improving Research Funding Efficiencies and Proposal Diversity , Institute for Progress, 2 February. Return to text
- Norton, A. 2024, Australia made 9 changes to student migration rules over the past year. We don’t need international student caps as well , The Conversation, August 5. Return to text