Report on Government Services 2023
PART F, SECTION 14: RELEASED ON 24 JANUARY 2023
14 Aged care services
This section focuses on government funded care and support services for older people and their carers, which are provided at home, in the community and in residential care facilities.
The Indicator results tab uses data from the data tables to provide information on the performance for each indicator in the Indicator framework. The same data are also available in CSV format.
Data downloads
- 14 Aged care services data tables (XLSX - 631 Kb)
- 14 Aged care services dataset (CSV - 1732 Kb)
See the corresponding table number in the data tables for detailed definitions, caveats, footnotes and data source(s).
- Context
- Indicator framework
- Indicator results
- Indigenous data
- Explanatory material
Objectives for aged care services
The aged care system aims to promote the wellbeing and independence of older people (and their carers), by enabling them to stay in their own homes or assisting them in residential care. Governments seek to achieve this aim by subsidising aged care services that are:
- accessible — including timely and affordable
- appropriate to meet the needs of clients — person-centred, with an emphasis on integrated care, ageing in place and restorative approaches
- high quality and safely delivered.
Governments aim for aged care services to meet these objectives in an equitable and efficient manner.
Service overview
As people age, they may need care and support to maintain health, social connectedness, wellbeing and independence to remain in their homes and communities. Around two in five older people reported being in need of assistance as they aged (ABS 2019). Family members, friends and neighbours provide much of the care and support for older people (ABS 2019). But not everyone’s care needs can be met through informal care and support. Around 80 per cent of older people will access some form of government funded aged care service before death (AIHW 2018).
Government funded aged care services are provided to older people who would like them and who have been assessed as in need of them. Services assist people who can no longer live without support to access appropriate care in their home, in the community or in a residential care facility. Approved aged care service providers receive government funding to provide these services and are required to meet minimum standards as well as demonstrate commitment to continuous improvement in quality of care.
Roles and responsibilities
Regulation and policy oversight of aged care services are predominantly the role of the Australian Government. The Aged Care Act 1997 (Cth) and the accompanying Aged Care Principles are the main regulatory instruments establishing the framework for aged care services in Australia. Provisions of the Act cover service planning, user rights, eligibility for care, funding, quality assurance and accountability and other matters. There are also a number of independent statutory bodies that have important responsibilities in relation to aged care services: the Aged Care Quality and Safety Commission, the Independent Health and Aged Care Pricing Authority, and the National Aged Care Advocacy Program. In addition, the Aged Care Sector Committee advises the Australian Government on aged care policy development and implementation, including quality in aged care (Aged Care Sector Committee 2020).
The Australian Government funds State and Territory Governments to provide comprehensive assessment services through the day-to-day operation and administration of Aged Care Assessment Teams (ACAT). While ACAT undertake comprehensive assessments for services under the Aged Care Act, lower entry-level service needs are assessed by Australian Government funded Regional Assessment Services (RAS).
The Australian Government funds residential aged care, home care and home support, with State, Territory and local governments also funding and/or delivering some of these services directly — for example, a small proportion of residential aged care facilities are owned by State and Territory governments. However, most services are delivered by non-government providers (tables 14A.10−11) such as private-for-profit, religious and charitable organisations.
The Australian Government and State and Territory Governments jointly administer/fund the Transition Care and Multi-Purpose Service (MPS) programs.
While the Australian Government subsidises a significant portion of the cost of providing aged care, clients and residents are expected to contribute where they can and may be charged fees by service providers.
Funding
In 2021-22, government recurrent expenditure on aged care services was $25.1 billion or $5570 per older person (table 14A.4 and figure 14.1). Residential and flexible care services accounted for the largest proportion of expenditure in 2021-22 ($15.8 billion, or 62.9 per cent). Home care and home support services accounted for much of the remainder ($8.3 billion) (table 14A.3).
The Australian Government provided 98.6 per cent of government funding for aged care services in 2021-22. State and Territory Governments provided the remainder (table 14A.3). Detailed expenditure data by program are contained in tables 14A.3-8.
Size and scope
Aged care target population
Demand for aged care services is driven by the size and health of the older population. The Australian population is ageing rapidly, with the proportion of people aged 65 years or over in the total population projected to increase from 15 per cent at 30 June 2017 to between 21 and 23 per cent in 2066 (ABS 2018a). Although the Aboriginal and Torres Strait Islander population is also ageing, life expectancy at birth for Aboriginal and Torres Strait Islander people is lower when compared with the non-Indigenous population (ABS 2018b).
The aged care target population is defined as all people aged 65 years or over and Aboriginal and Torres Strait Islander people aged 50–64 years (this aligns with the funding arrangements as specified under the National Health Reform Agreement). The aged care target population differs from the Australian Government’s aged care ‘planning population’ of people aged 70 years or over which is used, along with the population of Aboriginal and Torres Strait Islander people aged 50–69 years in some cases, to allocate places under the Aged Care Act. See the 'Explanatory material' tab for a definition of the aged care planning population.
Types of care and support
Home care and home support
Governments provide services to help older people remain or return to their homes. Carers can also access respite care through home care and home support programs:
- the Commonwealth Home Support Programme (CHSP) helps older people to access entry-level support services to remain living independently and safely at home and in their community. Services available under the CHSP include domestic assistance, personal care, social support, allied health and respite services. Table 14A.19 provides a full list of CHSP services.
- the Home Care Packages Program helps people with complex care needs to live independently in their own homes. There are four levels of care ranging from low level care needs (Home Care Package Level 1) to high care needs (Home Care Package Level 4). Services provided under these packages are tailored to the individual and might include personal care (such as showering), support services (such as cleaning) and/or clinical care (such as nursing and allied health support). As at 30 June 2022, 215 743 people were recipients of Home Care Packages, of which 41.2 per cent received a Home Care Package Level 2 (table 14A.9).
- Department of Veterans’ Affairs (DVA) community care for eligible veterans — Veteran Home Care (VHC) services provide domestic assistance, home and garden maintenance, and respite for people with low care needs; DVA community nursing services provide acute/post-acute support and maintenance and palliative care for people with high care needs or disability. In 2021-22, 33 192 veterans aged 65 years and over were approved for VHC services (a decrease of 7.0 per cent compared to 2020-21) and 10 726 veterans aged 65 years and over received community nursing services (a decrease of 15.1 per cent compared to 2020-21). VHC and community nursing service user numbers represent approximately 28.7 and 9.3 per cent of older eligible veterans respectively (table 14A.7-8).
In 2021-22, there were 808 722 older CHSP clients nationally, equivalent to around 179.4 older clients per 1000 older people (figure 14.2). There were a further 259 870 older clients of Home Care Packages, equivalent to around 57.7 older clients per 1000 older people (table 14A.2).
Residential care services
Residential aged care is provided in aged care homes on a permanent or respite basis. Residents receive accommodation, support (cleaning, laundry and meals) and personal care services (such as assistance with showering and toileting). Residents who have been assessed as requiring it may also receive mobility aids, continence products and tailored therapy services, as well as more complex nursing care.
For permanent residents, the Aged Care Funding Instrument (ACFI) is used to appraise care needs and the annual subsidy available through the Australian Government. Residents can be reappraised as their care needs change. Respite residents are not appraised under the ACFI but are classified as high or low care based on their ACAT approval. Information about the ACFI and the Average annual Australian Government subsidy can be found in table 14A.12. On 1 October 2022, the Australian National Aged Care Classification (AN-ACC) residential care funding model replaced the ACFI (Department of Health and Aged Care 2022a).
Information about usage rates per 1000 people by age and sex in permanent residential aged care and home care can be found in table 14A.17. Information on the proportion of permanent new residents and permanent resident care days by concessional, assisted, supported or low means can be found in table 14A.18.
The planning framework for services provided under the Aged Care Act aims to keep the growth in residential aged care places in line with growth in the older population, and to ensure a balance of services across Australia, including services for people with lower levels of need and in rural and remote areas. Up until February 2017, Home care places were also allocated under this framework. Under the Increasing Choices initiative introduced 27 February 2017, Home Care Packages are allocated to consumers rather than providers (consumers then choose a provider). At the same time, short-term restorative care places were introduced and are important in ensuring access to services across geographic locations.
Nationally at 30 June 2022, there were 72.1 residential care places per 1000 people in the aged care planning population (that is, aged 70 years or over) (table 14A.14). If the population of Aboriginal and Torres Strait Islander people aged 50–69 years is taken into account, the rate is 69.1 per 1000 older people (table 14A.15). This rate is higher in major cities (74.0) compared to regional areas (61.5) and remote/very remote areas (38.5) (tables 14A.16).
The rate of residential aged care places per 1000 people in the aged care planning population has been trending downwards over the past 10 years (84.5 per 1000 people in 2013) (table 14A.14). This might suggest that available residential aged care places are not keeping up with growth in the population of older people. Alternatively, it might indicate a preference for home-based care. Nationally, the number of home care package recipients has increased by around 170 per cent between 30 June 2016 and 30 June 2022 (table 14A.9).
During 2021-22, 242 377 older people were in permanent care (53.8 per 1000 older people) and 70 358 in respite care (15.6 per 1000 older people) (table 14A.2 and figure 14.3). At 30 June 2022, the occupancy rate for residential aged care was 86.2 per cent — the lowest rate over the 10 years of reported data (table 14A.13).
Flexible care services
Where mainstream residential or home care services are unable to cater for an older person’s specific needs, flexible care options are available:
- Transition Care provides goal-oriented and therapy-focused care on a time-limited basis to older people after a hospital stay, to help maximise their independence and minimise functional decline, thereby avoiding premature entry into residential aged care. During 2021-22, there were 21 349 older clients of Transition Care (table 14A.2).
- Short-term restorative care (STRC) is similar to transition care. It aims to improve the physical functioning, wellbeing and independence of older people, but without the need to have been in hospital. In 2021-22, 7411 people aged 65 years or over received STRC services, with 1271 people receiving care at 30 June 2022 (Department of Health and Aged Care 2022b).
- The MPS program delivers flexible and integrated health and aged care services to older Australians living in small communities in regional and remote areas. The MPS program provides health and aged care services in areas that cannot support both a hospital and a separate aged care home. At 30 June 2022 there were 3663 operational MPS program places (Department of Health and Aged Care 2022b).
- The National Aboriginal and Torres Strait Islander Flexible Aged Care Program funds services to provide flexible, culturally appropriate aged care to older Aboriginal and Torres Strait Islander people close to their home and/or community. Services funded under this program can deliver a mix of residential and home care services. At 30 June 2022, there were 1310 operational flexible places under this program with 475 in Flexible Residential Aged care (Department of Health and Aged Care 2022b).
Supporting programs
Governments fund ‘Workforce and Quality’ and ‘Ageing and Service improvement’ programs to monitor compliance with accreditation and quality frameworks and ensure appropriately skilled staff are available to deliver home and residential care services (including appropriate training to address a predicted rise in the prevalence of dementia). Staff providing home and residential care, and the physical environment at residential facilities, are critical to the health, safety and client experience of care and support. In 2021-22, the Australian Government spent $729.7 million on 'Workforce and Quality' and 'Ageing and Service Improvement' supports (table 14A.3).
The Aged Care Act does not prescribe the qualifications required by staff nor the number of staff required to be employed by an aged care service (Department of Health and Aged Care 2018), but the Aged Care Quality Standards include a mandatory human resources standard for all government funded aged care providers. Standard 7 requires aged care providers to employ staff with the right skills and qualifications to provide care and that aged care client interactions should be kind, caring and respectful of an older person's identity, culture, and diversity. Table 14A.37 provides data on the proportion of assessed aged care providers that met the Aged Care Quality Standards.
The physical environment at residential facilities is assessed as part of ongoing accreditation processes by the Aged Care Quality and Safety Commission (tables 14A.34–37).
Providers have responsibility for ensuring that their workforce upholds the rights of clients and residents as outlined in the Charter of Aged Care Rights.
In 2020, 27.9 per cent of full time equivalent (FTE) direct care staff at aged care homes were either nurses or allied health professionals, down from 28.5 per cent in 2016 (Department of Health and Aged Care 2017a, 2021a).
Accessing care
Information services
Services such as ‘My Aged Care’ provide older people, their families and carers with information to help them access timely and appropriate care and find approved aged care services in their local area.
Assessment services
An assessment of need by an ACAT (Aged Care Assessment Service in Victoria), is mandatory for admission to residential care, to receive a Home Care Package, or enter STRC or Transition Care. ACATs also make recommendations regarding the most appropriate long-term care arrangements for clients (table 14A.27). Since 2014, care approvals from most assessments do not lapse. Assessments for other aged care programs are primarily conducted by other assessment services (for example, Regional Assessment Services (RAS) for CHSP).
Not everyone assessed by an ACAT is approved for care, and some people are approved for more than one type of care. Nationally in 2021-22, there were 200 865 completed ACAT assessments (equivalent to 44.6 per 1000 older people) (table 14A.20) and 237 226 approvals for residential aged care and the Home Care Package program for people aged 65 years and over (tables 14A.20–21). ACAT approval rates increase significantly with client age (table 14A.21).
Elapsed times — time taken from ACAT approval to access care
The time between an ACAT approval and an older person’s access to an aged care service (or offer of a package in the case of Home Care, as distinct from access to care) can be influenced by a range of factors (both service- and person-related) including:
- availability of places/packages and services (which can increase waiting times)
- an older person’s:
- preference to remain at home for as long as possible, going into approved residential aged care at a later date or not at all (choosing instead to access formal home care, or support from family, friends or the community)
- need to delay entry into residential aged care due to personal circumstances, such as selling their home
- decision to reject an offer due to the cost or location.
For Home Care Packages, once the assignment of a Package has been made, a client has 56 calendar days to enter into a Home Care Agreement with an approved provider. Clients are able to apply for an extension of 28 days, giving them a total of 84 calendar days in which to enter into an agreement with a provider. This time period is not captured in the elapsed times data for Home Care Packages reported below.
If a client has not entered into a Home Care Agreement by the required time, their Home Care Package will be withdrawn. If the client later decides that they want to receive home care services, they can rejoin the National Priority System (NPS). They will re-enter the NPS based on their approval date and are not disadvantaged (Department of Health and Aged Care 2017b).
In 2021-22, 40.8 per cent of older people entered residential aged care within 3 months of their ACAT approval (figure 14.4); the median elapsed time was 153 days, a decrease from 163 days in 2020-21 (table 14A.22). Nationally, the median elapsed time between ACAT approval and entry into aged care services increased by around 282.5 per cent (an almost fourfold increase) between 2012-13 and 2021-22. Further data on elapsed times for residential aged care are included in tables 14A.24–26.
Nationally in 2021-22, median elapsed times for assignment of a Home Care Package for all priority groups ranged from 1 month for a Level 4 package to 8 months for a Level 2 or 3 package, a decrease compared to 2020-21 (figure 14.5).
The performance indicator framework provides information on equity, effectiveness and efficiency, and distinguishes the outputs and outcomes of aged care services.
The performance indicator framework shows which data are complete and comparable in this Report. For data that are not considered directly comparable, text includes relevant caveats and supporting commentary. Section 1 discusses data comparability and completeness from a Report-wide perspective. In addition to the contextual information for this service area (see Context tab), the Report’s statistical context (section 2) contains data that may assist in interpreting the performance indicators presented in this section.
Improvements to performance reporting for aged care services are ongoing and include identifying data sources to fill gaps in reporting for performance indicators and measures, and improving the comparability and completeness of data.
Outputs
Outputs are the services delivered (while outcomes are the impact of these services on the status of an individual or group) (see section 1). Output information is also critical for equitable, efficient and effective management of government services.
Outcomes
Outcomes are the impact of services on the status of an individual or group (see section 1).
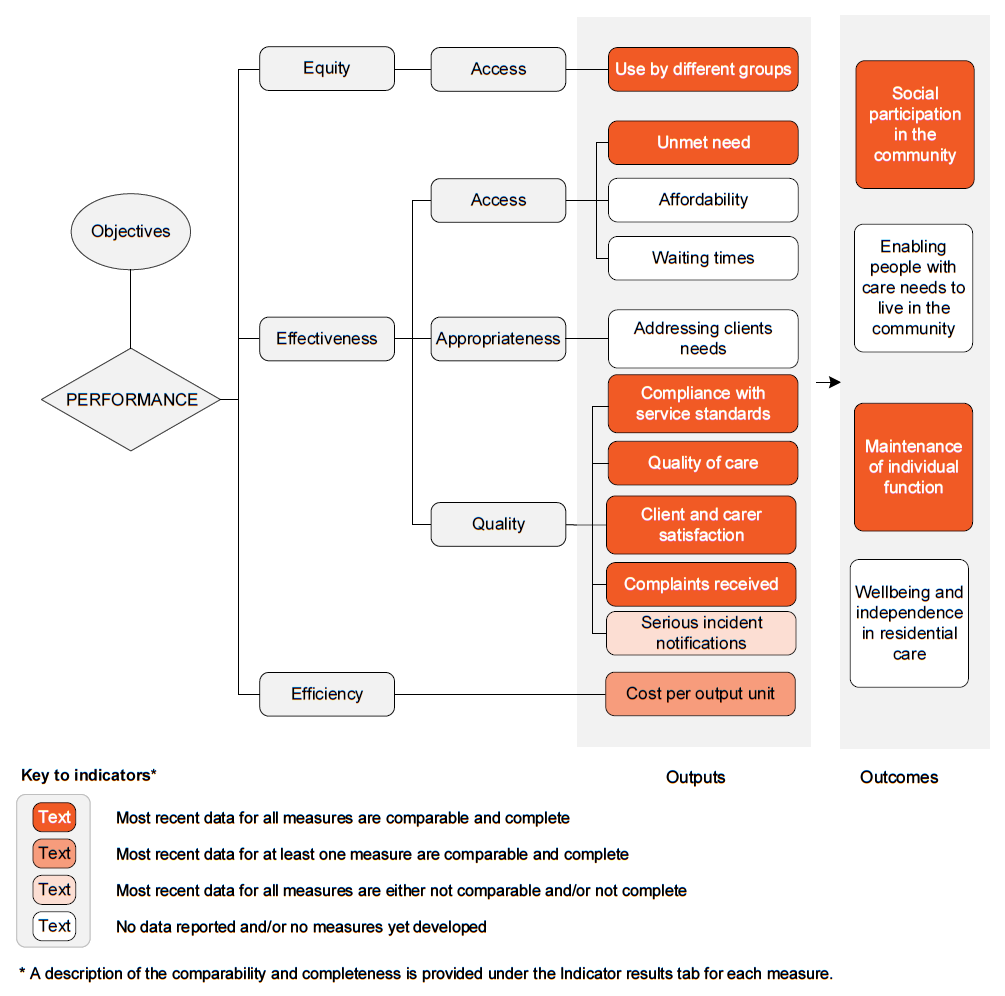
Text version of indicator framework
Performance — linked to Objectives
Outputs
- Equity — Access
- Use by different groups – most recent data for all measures are comparable and complete
- Effectiveness — Access
- Unmet need – most recent data for all measures are comparable and complete
- Affordability – no data reported and/or no measures yet developed
- Waiting times – no data reported and/or no measures yet developed
- Effectiveness — Appropriateness
- Addressing client needs – no data reported and/or no measures yet developed
- Effectiveness — Quality
- Compliance with service standards – most recent data for all measures are comparable and complete
- Quality of care – most recent data for all measures are comparable and complete
- Client and carer satisfaction – most recent data for all measures are comparable and complete
- Complaints received – most recent data for all measures are comparable and complete
- Serious incident notifications – most recent data for all measures are either not comparable and/or not complete
- Efficiency — Inputs per output unit
- Cost per output unit – most recent data for at least one measure are comparable or complete
Outcomes
- Social participation in the community – most recent data for all measures are comparable and complete
- Enabling people with care needs to live in the community – no data reported and/or no measures yet developed
- Maintenance of individual function – most recent data for all measures are comparable and complete
- Wellbeing and independence in residential care – no data reported and/or no measures yet developed
A description of the comparability and completeness is provided under the Indicator results tab for each measure.
This section presents an overview of 'Aged care services' performance indicator results. Different delivery contexts, locations and types of clients can affect the equity, effectiveness and efficiency of aged care services.
Information to assist the interpretation of these data can be found with the indicators below and all data (footnotes and data sources) are available for download above as an excel spreadsheet and as a CSV dataset. Data tables are identified by a ‘14A’ prefix (for example, table 14A.1).
Specific data used in figures can be downloaded by clicking in the figure area, navigating to the bottom of the visualisation to the grey toolbar, clicking on the 'Download' icon and selecting 'Data' from the menu. Selecting 'PDF' or 'Powerpoint' from the 'Download' menu will download a static view of the performance indicator results.
1. Use by different groups
‘Use by different groups’ is an indicator of governments’ objective to subsidise aged care services in an equitable manner.
‘Use by different groups’ is defined as the proportion of service clients who are from a selected equity group, compared with the proportion of the aged care target population who are from that selected equity group.
The proportion of service clients from a particular selected equity group should be broadly similar to the proportion of the aged care target population who are from that selected equity group.
There are nine selected equity groups identified by the Aged Care Act 1997 (Cth) (referred to as 'special needs' groups in the Act; see the 'Explanatory material' tab for details). Data are reported for three selected equity groups (Aboriginal and Torres Strait Islander people; people from Culturally and Linguistically Diverse (CALD) backgrounds; and people receiving aged care services in outer regional, remote/very remote areas). People from CALD backgrounds are defined as those born overseas from countries other than the United Kingdom, Ireland, New Zealand, Canada, South Africa and the United States of America.
Measures for veterans (including widows and widowers of veterans) and for people who are financially and socially disadvantaged are currently under development (although data are available on the proportion of all permanent residents’ care days used by financially disadvantaged residents, see table 14A.18). Data are not available for reporting on the remaining selected equity groups.
Several factors should be considered when interpreting these data.
- Selected equity groups may have greater need for aged care services. Compared to the rest of the population, Aboriginal and Torres Strait Islander people have higher rates of disability, lower life expectancy and an increased likelihood of requiring aged care services at a younger age. Because of these factors, the target population for Aboriginal and Torres Strait Islander people is people aged 50 years and over, compared to 65 years and over for other population groups.
- Cultural differences and the availability of care and support from family, friends and neighbours can also affect the use of services across different population groups. Stronger support networks can reduce the need for government funded aged care services, or for particular government funded service types.
Differences in the representation of a selected equity group in services compared to their representation in the aged care target population varied across service types and groups. Nationally in 2021-22:
- Aboriginal and Torres Strait Islander people were underrepresented in all service types, but less so for Home Care Packages
- people from CALD backgrounds were overrepresented among people accessing Home Care Packages and the Aged Care Assessment Program, but underrepresented in all other service types
- people receiving aged care services in rural and remote areas were overrepresented among people accessing CHSP but underrepresented in all other service types.
2. Unmet need
‘Unmet need’ is an indicator of governments’ objective to subsidise aged care services that are accessible.
‘Unmet need’ measures aged care service access relative to need. Two measures of unmet need are reported.
Unmet need in the community
‘Unmet need in the community’ measures the proportion of older people (aged 65 years and over) living in households who reported being in need of assistance, and whose need for assistance was not fully met.
A low or decreasing proportion of people reporting their need for assistance as not fully met is desirable.
Data for the NT should be interpreted with caution as the Survey of Disability, Ageing and Carers excludes very remote areas which comprises more than 20 per cent of the estimated resident population in the NT living in private dwellings.
Hospital patient days used by aged care type patients
‘Hospital patient days used by aged care type patients’ is a proxy measure of unmet need defined as the proportion of hospital patient days (for overnight separations only) that were for aged care type patients (see 'Explanatory material' tab for further details).
Hospital inpatient services are geared towards shorter periods of acute care aimed at addressing serious illness or injury, or diagnosis. The needs of older people for maintenance care (particularly for extended periods of time) can be better met in residential aged care services than hospitals.
Understanding the relationship between the aged care and health systems is important as interactions are critical for the performance of both systems. The number of operational residential aged care places can affect demand for public hospital beds, just as the number of older patients in acute and subacute care and the time they spend in hospital can affect demand for aged care services.
A low or decreasing proportion of patient days used by aged care type patients is desirable.
These data should be interpreted with caution, because:
- days for patients who have not completed their period of care in a hospital are not included
- identification in hospital as an aged care patient type may not reflect a person’s eligibility for residential care services (this is determined by an ACAT assessment) or reliably reflect access issues for residential aged care from the acute care sector — linked ACAT and hospital separations data are not available at this time
- the diagnosis codes for aged care patient type may not be applied consistently across jurisdictions or over time
- the denominator (all patient days for overnight separations) does not directly reflect the need for aged care services
- the scope of aged care type patients differs slightly to the equivalent National Healthcare Agreement indicator (see table 14A.32 for details).
Nationally in 2018, 34.0 per cent of older people who were living in households and in need of assistance reported that their need was not fully met (figure 14.6a). The proportion was higher for older people with a profound or severe disability (41.7 per cent) than for older people without a disability (20.5 per cent) (table 14A.31).
Nationally in 2020‑21, the rate of all hospital patient days used by patients waiting for residential aged care was 9.2 per 1000 patient days (figure 14.6b). Rates were lower for Aboriginal and Torres Strait Islander people compared to other Australians, but higher for people from lower compared to higher socioeconomic areas and for people in remote compared to non‑remote areas (table 14A.33). The proportion of separations for ‘aged care type’ patients waiting 35 days or longer was 9.8 per cent nationally in 2020-21 (table 14A.32).
3. Affordability
‘Affordability’ is an indicator of governments’ objective to subsidise aged care services to improve affordability for people who need them.
‘Affordability’ is defined as out‑of‑pocket costs for aged care services (after subsidies), as a proportion of disposable income.
Low or decreasing out‑of‑pocket cost for aged care services as a proportion of disposable income represents more affordable aged care services and is desirable.
Data are not yet available for reporting on this indicator.
4. Waiting times
‘Waiting times’ is an indicator of governments’ objective to subsidise aged care services that are accessible.
‘Waiting times’ is defined as the proportion of older people who have an ACAT approval and are ready to take up care, who are able to enter residential care or commence home care within three months.
Higher proportions of admission to residential care or commencement of home care within three months are desirable.
Data are not yet available for reporting on this indicator.
Elapsed times between approval for care and (1) entry into residential aged care and (2) assignment of home care are reported in the 'Context' section.
5. Addressing client needs
‘Addressing client needs’ is an indicator of governments’ objective to subsidise aged care services that are appropriate to meet the needs of clients — person‑centred, with an emphasis on integrated care, ageing in place and restorative approaches.
‘Addressing client needs’ will measure the extent to which:
- care recipients or their representatives had input into the planning of their care
- the supports identified in the care planning process to address an individual’s needs were provided (match of needs)
- individual interests, customs, beliefs and cultural and ethnic backgrounds were valued and fostered.
Data are not yet available for reporting on this indicator.
6. Compliance with service standards
‘Compliance with service standards’ is an indicator of governments’ objective to subsidise high quality aged care services.
‘Compliance with service standards’ measures the extent to which approved aged care services are meeting expected standards. Measures are reported for residential care and home care and home support.
Residential care — re-accreditation
For residential aged care, the proportion of accredited facilities given three‑year re-accreditation is reported. Three years is the longest period for which re‑accreditation can be granted (in most cases), so if a service is re‑accredited for this period it implies a higher level of service quality than for those re‑accredited for a shorter period. Further information on the accreditation standards and process is available at www.agedcarequality.gov.au.
Data for this measure do not include new facilities (0.8 per cent of all residential care facilities) that have not been re‑accredited as at 30 June 2022 (table 14A.37).
High or increasing proportions of services that are re‑accredited for three years are desirable.
Compliance with Aged Care Quality Standards
On 1 July 2019, the Aged Care Quality Standards took effect for organisations providing all types of Commonwealth‑subsidised aged care services.
- Standard 1 — Consumer dignity and choice
- Standard 2 — Ongoing assessment and planning with consumers
- Standard 3 — Personal care and clinical care
- Standard 4 — Services and supports for daily living
- Standard 5 — Organisation’s service environment
- Standard 6 — Feedback and complaints
- Standard 7 — Human resources
- Standard 8 — Organisational governance.
High or increasing proportions of services that met all expected outcomes are desirable.
During 2021‑22, 85.0 per cent of the 938 services re‑accredited that year were given three-year accreditation status; up from 75.5 per cent in 2020‑21 (table 14A.34). At 30 June 2022, 86.1 per cent of all 2640 re‑accredited residential aged care services had been given three-year accreditation, continuing a downward trend in the proportion of services given three-year re-accreditation over the 10 years of available data (95.7 per cent at 30 June 2013) (figure14.7 and table 14A.37).
For Australian Government subsidised aged care services, 26.6 per cent of services received a re-accreditation audit during 2021-22 for residential aged care services, and 8.5 per cent received a quality audit for home care and support (table 14A.38). The proportions of residential aged care and home care and home support service providers reviewed during 2021‑22 that achieved the standards are in table 14.2.
7. Quality of care
‘Quality of care’ is an indicator of governments’ objective to subsidise high quality aged care services. High quality aged care services provide services that meet residents’ personal, functional, clinical and psycho-social needs to a high standard.
‘Quality of care’ in residential aged care services is measured according to the expanded National Aged Care Mandatory Quality Indicator Program. Participation in the National Aged Care Mandatory Quality Indicator Program has been a requirement for all Australian Government subsidised residential aged care services since 1 July 2019.
Since 1 July 2021, approved providers of residential aged care are required to report on five quality indicators. The definitions and data collection methods for each quality indicator are outlined in the National Aged Care Mandatory Quality Indicator Program Manual 2.0 (Department of Health and Aged Care 2021).
The indicator is defined by five measures:
- Pressure injuries
- Physical restraint
- Unplanned weight loss
- Falls and major injury
- Medication management.
Further details on the definitions of these measures are available in the Key terms section.
All else being equal, a low or decreasing occurrence of pressure injuries, use of physical restraint, unplanned weight loss, falls and polypharmacy can suggest higher quality services. However, high or increasing occurrences might reflect more effective reporting and monitoring arrangements.
National program percentages for the 2021-22 period were as follows:
Pressure injuries – care recipients were observed for pressure injury once each quarter during 2021-22. In quarter 4 (Q4; April to June 2022), 6.3 per cent of care recipients had one or more pressure injuries, prevalence was higher for lower grade pressure injuries. Data were similar across all quarters (between 5.7 per cent and 6.3 per cent of care recipients with one or more pressure injuries in Q2 and Q4, respectively) (table 14A.39).
Physical restraint – the use of physical restraint was assessed by reviewing three days of existing care records each quarter during 2021-22. In quarter 4 (Q4; April to June 2022), 21.6 per cent of care recipients experienced physical restraint, 17.1 per cent were restrained exclusively through the use of a secure area. Data were similar across all quarters: for care recipients who experienced physical restraint (between 21.2 per cent and 22.7 per cent in Q3 and Q1, respectively) and for care recipients who experience physical restraint through the use of a secure area (between 16.6 per cent and 17.3 per cent in Q3 and Q1, respectively) (table 14A.40).
Unplanned weight loss – assessment of care recipients’ weight loss occurred monthly, however both unplanned weight loss indicators were measured on a quarterly basis during 2021-22. In quarter 4 (Q4; April to June 2022), 9.4 per cent of care recipients experienced significant unplanned weight loss (meaning unplanned weight loss of 5.0 per cent or more when comparing their current and previous quarter finishing weights) and 9.4 per cent of care recipients experienced consecutive unplanned weight loss (meaning consecutive unplanned weight loss every month over three consecutive months of the quarter). Data showed some variation across quarters: for care recipients who experienced significant unplanned weight loss (between 8.4 per cent and 10.8 per cent in Q1 and Q3, respectively) and for care recipients who experienced consecutive unplanned weight loss (between 9.4 per cent and 11.1 per cent in Q4 and Q3, respectively) (table 14A.41).
Falls and major injury – falls and falls resulting in major injury were assessed by reviewing care records over the entire quarter for each quarter during 2021-22. In quarter 4 (Q4; April to June 2022), 32.2 per cent of care recipients experienced a fall with 2.2 per cent resulting in major injury (for example, bone fractures, joint dislocations, and head injuries). Data were similar across all quarters: for care recipients who experienced a fall (between 31.6 per cent and 32.2 per cent in Q3 and Q4, respectively) and for care recipients who experienced a fall resulting in major injury (between 2.1 per cent and 2.2 per cent in Q1-Q3 and Q4, respectively) (table 14A.42).
Medication management – care recipients' medication charts and/or records were assessed through a single review each quarter during 2021-22. In quarter 4 (Q4; April to June 2022), 37.5 per cent of care recipients were prescribed nine or more medications. In Q4, 10.7 per cent of all care recipients received antipsychotic medications for a diagnosed condition of psychosis, although 19.7 per cent of all care recipients received antipsychotic medications. Data showed some variation across quarters: for care recipients who were prescribed nine or more medications (between 37.5 per cent and 40.6 per cent in Q3-Q4 and Q1, respectively) and for care recipients who received antipsychotics (between 19.7 per cent and 21.2 per cent in Q4 and Q1, respectively) (table 14A.43).
National Aged Care Mandatory Quality Indicator Program data used to report on this indicator are based on quarterly assessment data recorded by service as distinct from care recipients. Therefore, it is not possible to determine the number of quarters in which the same care recipients were assessed.
8. Client and carer satisfaction
‘Client and carer satisfaction’ is an indicator of governments' objective to subsidise high quality aged care services.
‘Client and carer satisfaction’ is defined by four measures:
- the proportion of people aged 65 years or over living in households, who are satisfied with the range of organised and formal service options available
- the proportion of people aged 65 years or over living in households, who are satisfied with the quality of assistance received from organised and formal services in the last six months
- the proportion of primary carers living in households (caring for people aged 65 years or over), who are satisfied with the range of formal service options available to help them in their caring role
- the proportion of primary carers living in households (caring for people aged 65 years or over), who are satisfied with the quality of assistance received from formal services in the last six months to help them in their caring role.
A high or increasing proportion of clients and carers who are satisfied is desirable as it suggests that the service received was of a higher quality.
Data for the NT should be interpreted with caution as the Survey of Disability, Ageing and Carers excludes very remote areas which comprises more than 20 per cent of the estimated resident population in the NT living in private dwellings.
Nationally in 2018, 71.2 per cent of people aged 65 years and over who reported a need for, or received formal services in the previous six months, were satisfied with the range of services available — a decrease from 2015, but similar to 2012 (figure 14.9a).
Of people aged 65 years or over who received formal services in the previous six months, 84.4 per cent were satisfied with the quality of assistance they received (table 14A.48) — a decrease from 2015 and 2012 (89.2 per cent and 88.6 per cent respectively).
For primary carers of people aged 65 years or over, the proportion who were satisfied with the range of organised services available to help them in their caring role was 36.1 per cent in 2018 — a decrease of around 10 percentage points from 2015 and 2012 (figure 14.9b).
Around 7 in 10 primary carers (71.3 per cent) were satisfied with the quality of services provided to help them in their caring role — down from 84.7 per cent in 2012 (table 14A.50).
9. Complaints received
‘Complaints received’ is an indicator of governments’ objective to subsidise high quality aged care services.
‘Complaints received’ is defined as the number of in‑scope complaints received by the Aged Care Quality and Safety Commission for residential aged care services per 1000 residential aged care residents (permanent and respite). Complaints within scope relate to Australian Government funded providers of residential care, Home Care, CHSP or flexible aged care services.
All else being equal, a low or decreasing rate of complaints can suggest higher quality services. However, a high or increasing rate of complaints may not necessarily mean lower quality services. It may reflect more effective complaints reporting and monitoring arrangements.
Further information on the operation of the Aged Care Quality and Safety Commission is available at www.agedcarequality.gov.au.
During 2021‑22, the Aged Care Quality and Safety Commission received 10 326 in‑scope complaints (6406 concerned permanent and respite residential aged care services), equivalent to 34.0 complaints per 1000 residential care residents, similar to the rate in 2020-21 (figure 14.9).
10. Serious incident notifications
‘Serious incident notifications’ is an indicator of governments’ objective to subsidise high quality aged care services.
‘Serious incident notifications’ is defined as the number of Serious Incident Response Scheme notifications received by the Aged Care Quality and Safety Commission, by primary incident type, per 10 000 occupied bed days in residential care.
The Serious Incident Response Scheme (the Scheme) was introduced on 1 April 2021. The purpose of the Scheme is to help prevent and reduce incidents of abuse and neglect in residential aged care services subsidised by the Australian Government.
The Scheme requires aged care providers to:
- manage and take reasonable action to prevent incidents with a focus on the safety, health, wellbeing and quality of life of older people in residential aged care
- have an effective incident management system to respond to, assess, and enable continuous improvement to their management and prevention of incidents
- notify all reportable incidents to the Aged Care Quality and Safety Commission. Reportable incidents include any of the below that have occurred, are alleged to have occurred, or are suspected of having occurred to a consumer in residential care, in connection with the provision of residential or flexible care in a residential setting:
- unreasonable use of force
- unlawful sexual contact or inappropriate sexual conduct
- neglect
- psychological or emotional abuse
- unexpected death
- stealing or financial coercion by a staff member
- inappropriate use of restrictive practices
- unexplained absence from care
Low or decreasing rates of Serious incident notifications are desirable. However, high or increasing rates might reflect more effective incident reporting mechanisms and organisational cultural change.
The number of Serious incident notifications does not necessarily correlate to the number of instances of harm to an older person in aged care. Reports might include multiple notifications of the same matter, allegations of incidents, and situations where incidents occurred but injury was avoided. Incident rates should be monitored over time to identify trends.
Only national data for the 2021-22 period were provided for publication in this Report for the first time. It is expected that state and territory data will be available for future Reports.
Nationally, during 2021-22, the Aged Care Quality and Safety Commission received 37 833 Serious Incident Response Scheme notifications from residential aged care services providers, equating to 5.5 notifications per 10 000 occupied bed days. Notifications most commonly concerned the unreasonable use of force (table 14A.53).
11. Cost per output unit
‘Cost per output unit’ is an indicator of governments’ objective to subsidise aged care services in an efficient manner.
‘Cost per output unit’ is defined by two measures:
- Australian Government expenditure per ACAT assessment — Australian Government expenditure on the Aged Care Assessment Program divided by the number of completed assessments
- expenditure per hour of service for CHSP — Australian Government expenditure on services, divided by the number of hours of service provided.
While high or increasing cost per output unit may reflect deteriorating efficiency, it may also reflect changes in aspects of the service (such as greater time spent with clients) or differences in the characteristics of clients (such as their geographic location). Similarly, while low or declining cost per output unit may reflect improving efficiency it may also reflect declining quality.
Not all expenditure is included in these measures. Expenditure by local governments and non‑government sources on services (for example, client fees for CHSP) and State and Territory governments’ contributions to the cost of ACAT assessments are not included.
Efficiency (cost per unit) measures for residential care and home care are under development.
Nationally in 2021-22, average Australian Government expenditure per ACAT assessment was $662.71 (figure 14.12a).
Nationally in 2021-22, Australian Government expenditure on CHSP services per hour was higher for nursing and allied health than for domestic assistance and personal care (figure 14.12b and 14.12c).
‘Social participation in the community’ is an indicator of governments’ objective to encourage the wellbeing and independence of older people.
‘Social participation in the community’ is indicative of the wellbeing and independence of older people as defined by three measures, the estimated proportions of older people (aged 65 years and over) who:
- participated in social or community activities away from home in the last three months
- had face‑to‑face contact with family or friends not living in the same household in the last week
- did not leave home or did not leave home as often as they would like.
These measures are reported by disability status (profound or severe disability, other disability, all disability, without disability) and for all older people. Disability status is used as a proxy to identify older people who might need more assistance to support their social participation.
High or increasing proportions of social participation in the community are desirable.
Data for the NT should be interpreted with caution as the Survey of Disability, Ageing and Carers excludes very remote areas which comprises more than 20 per cent of the estimated resident population in the NT living in private dwellings.
Nationally in 2018:
- 94.4 per cent of older people reported having participated in social or community activities away from home in the last three months; similar to 2015 (figure 14.13)
- 77.1 per cent of older people reported having face‑to‑face contact with family or friends who were not living in the same household in the last week; similar to 2015 (table 14A.57)
- 13.8 per cent of older people reported they did not leave home or did not leave home as often as they would like; similar to 2015 (table 14A.58).
Data are available by disability status in tables 14A.56–58.
13. Enabling people with care needs to live in the community
‘Enabling people with care needs to live in the community’ is an indicator of governments’ objective to promote the wellbeing and independence of older people, by enabling them to stay in their own homes.
Enabling people with care needs to live in the community’ is defined as the proportion of older people with care needs who are living in the community.
An increasing proportion of older people with care needs who want to and are living in the community is desirable. This indicator should be considered alongside the outcome indicator on social participation.
Data are not yet available for reporting against this indicator.
14. Maintenance of individual function
‘Maintenance of individual function’ is an indicator of governments’ objective for aged care services to promote the wellbeing and independence of older people.
‘Maintenance of individual function’ is defined as improvement in the level of physical function for Transition Care Programme (TCP) clients from entry to exit, measured as the difference between the average Modified Barthel Index (MBI) score on TCP entry and exit.
An increase in the score from entry to exit is desirable.
The MBI is a measure of functioning ranging from 0 (fully dependent) to 100 (fully independent). Data are reported for recipients who completed a TCP episode only. See the context section for more information on TCP.
This indicator needs to be interpreted with caution. The TCP operates with some differences across jurisdictions including differences in health and aged care service systems, local operating procedures and client groups. Variation in the average MBI scores on entry and exit from the program may reflect differences in client groups for the program across jurisdictions. Only completed episodes of Transition Care are included in the calculations for this indicator.
The TCP is a small program only available directly upon discharge from hospital (in 2021‑22 there were 18 887 admissions to the TCP) (table 14A.59). The average duration is around ten weeks, with a maximum duration of 12 weeks (may be extended by a further 6 weeks in some circumstances).
Nationally in 2021‑22, the average MBI score for TCP clients increased from entry (71) to exit (82), similar to previous years. Entry and exit scores vary across jurisdictions (figure 14.14).
15. Wellbeing and independence in residential care
‘Wellbeing and independence in residential care’ is an indicator of governments’ objective to promote the wellbeing and independence of older people, by assisting them in residential care.
‘Wellbeing and independence in residential care’ is defined as the proportion of older people assessed as having a high quality of life in residential aged care. Quality of life is the degree to which an individual resident’s wellbeing meets their personal expectations and those of their carers.
A high or increasing proportion of older people in residential aged care with a high quality of life is desirable.
Data are not yet available for reporting on this indicator.
Performance indicator data for Aboriginal and Torres Strait Islander people in this section are available in the data tables listed below. Further supporting information can be found in the 'Indicator results' tab and data tables.
| Table number | Table title |
|---|---|
| Table 14A.26 | Elapsed times for residential aged care, by Indigenous status |
| Table 14A.29 | Representation of Aboriginal and Torres Strait Islander people in the aged care target population and aged care recipients |
| Table 14A.32 | Public hospital separations for care type 'maintenance' for older people aged 65 years or over and Aboriginal and Torres Strait Islander people aged 50-64 years |
| Table 14A.33 | Hospital patient days used by those eligible and waiting for residential aged care |
Key terms
| Terms | Definition |
|---|---|
Accreditation | Accreditation is a key component of the Australian Government’s quality framework for federally funded residential aged care and is a quality assurance system for residential aged care services — based on the principle of continuous improvement. Accreditation requires assessment against the Aged Care Quality Standards ‑ grouped into eight standards: consumer dignity and choice; ongoing assessment and planning with consumers; personal care and clinical care; services and supports for daily living; service environment; feedback and complaints; human resources; and organisational governance. |
Aged care | Services funded and/or provided by governments that respond to the functional and social needs of older people, and the needs of their carers. Home care and home support services aim to optimise independence and to assist older people to stay in their own homes, while residential care services provide accommodation and care for those who can no longer be cared for at home. Assessment of care needs is an important component of aged care. The majority of aged care services assist in activities of daily living such as personal care (for example, bathing and dressing), housekeeping and meal provision. Other services aim to promote social participation and connectedness. These services are delivered by trained aged care workers and volunteers. However, aged care services may also be delivered by health professionals such as nurses and occupational therapists. Aged care services generally aim to promote wellbeing and foster function rather than to treat illness. Although some aged care services such as transition care have a specific restorative role, they are distinguished from the health services described in Part E of this Report. Aged care services may be funded through programs specifically or mainly directed to older people, or through programs that address the needs of people of different ages. |
Aged care target population | The Aged Care target population is defined as all people (Aboriginal and Torres Strait Islander and non‑Indigenous) aged 65 years or over and Aboriginal and Torres Strait Islander Australians aged 50–64 years. This is the population within the scope of, and funded for services under, the national aged care system. |
Aged care type patient (unmet need indicator) | Aged care type patients are those who are waiting for residential aged care where the care type is Maintenance, a diagnosis was reported as Person awaiting admission to residential aged care service and the separation mode was not Other (includes discharge to place of usual residence). Includes overnight separations only. |
Aged care planning population | The Aged care planning population is defined as people aged 70 years or over. This is the population used by the Australian Government for its needs‑based planning framework to ensure sufficient supply of both places by matching the growth in the number of aged care places with growth in the aged population. It also seeks to ensure balance in the provision of services between metropolitan, regional, rural and remote areas, as well as between people needing differing levels of care. Under the framework, the Australian Government seeks to achieve and maintain a specified national provision level of subsidised operational aged care places for every 1000 people aged 70 years or over. This provision level is known as the aged care provision ratio (DoHA 2012). |
Aged Care Quality Standards | From 1 July 2019 organisations providing Australian Government subsidised aged care services have been required to comply with the Aged Care Quality Standards. Organisations are assessed by the Aged Care Quality and Safety Commission and must be able to provide evidence of their compliance with the eight standards (ACQSC 2020): Standard 1 — Consumer dignity and choice: this standard reflects concepts important in treating consumers with dignity and respect, supporting choice and independence, and fostering social inclusion, health and wellbeing. Standard 2 — Ongoing assessment and planning with consumers: planned care and services should meet each consumer’s needs, goals and preferences, and optimise their health and wellbeing. Standard 3 — Personal and clinical care: consumers and the community expect the safe, effective and quality delivery of personal and clinical care, applying to all services delivering personal and clinical care specified in the Quality of Care Principles. Standard 4 — Service and supports for daily living: covers a wide range of options that aim to support consumers to live as independently as possible. Standard 5 — Organisation’s service environment: applies to physical service environments that organisations provide for residential care, respite care and day therapy centres. Standard 6 — Feedback and complaints: requires an organisation to have a fair, accessible, confidential and prompt system for resolving complaints. Standard 7 — Human resources: requires an organisation to have and use a skilled and qualified workforce. Standard 8 — Organisational governance: this Standard holds the governing body of an organisation responsible for the organisation and delivery of safe and quality care services. Further detail on the standards can be found on the ACQSC website at https://agedcarequality.gov.au. |
Ageing in place in residential care | An approach that aims to provide residents with appropriate care and increased choice by allowing them to remain in the same facility regardless of changes in their level of care needs. It also allows couples with different levels of care needs to be cared for in the same facility. The main facet of ‘ageing in place’ is that funding is tied to the assessed care needs of the client rather than to the services provided by the facility. |
Capital expenditure on residential services | Expenditure on building and other capital items, specifically for the provision of Australian Government funded residential aged care. |
Care leaver | A care leaver is a person who was in institutional care (such as an orphanage or mental health facility) or other form of out‑of‑home care, including foster care, as a child or youth (or both) at some time during their lifetime (DoHA 2012). |
Centre‑based respite | Respite care provided from a facility such as a day care or health centre. Respite care is usually combined with social support services to maintain the functional capabilities of the person receiving care. |
Complaint | A complaint by the affected care recipient or his or her representative, or anyone else, to the ACQSC about matters relevant to an approved provider’s responsibilities under the Aged Care Act 1997 (Cth) or the Aged Care Principles. |
Disability | In the ABS SDAC 2018, a person has a disability if they report they have a limitation, restriction or impairment, which has lasted, or is likely to last, for at least six months and restricts everyday activities. This includes: loss of sight (not corrected by glasses or contact lenses); loss of hearing where communication is restricted, or an aid to assist with, or substitute for, hearing is used; speech difficulties; shortness of breath or breathing difficulties causing restriction; chronic or recurrent pain or discomfort causing restriction; blackouts, seizures, or loss of consciousness; difficulty learning or understanding; incomplete use of arms or fingers; difficulty gripping or holding things; incomplete use of feet or legs; nervous or emotional condition causing restriction; restriction in physical activities or in doing physical work; disfigurement or deformity; mental illness or condition requiring help or supervision; memory problems or periods of confusion causing restriction; social or behavioural difficulties causing restriction; long term effects of head injury, stroke or other brain damage causing restriction; receiving treatment or medication for any other long term conditions or ailments and still being restricted and any other long term conditions resulting in a restriction. |
Elapsed time | The measure of the time elapsed between an ACAT approval and entry into a residential care service or assignment of a Home Care Package. |
| National Aged Care Mandatory Quality Indicator Program | Pressure injuries:
Physical restraint:
Unplanned weight loss:
Falls and major injury:
Medication management:
|
Older people | All people (Aboriginal and Torres Strait Islander and non‑Indigenous) aged 65 years or over and Aboriginal and Torres Strait Islander Australians aged |
People from non‑English speaking countries | People who were born in non‑English speaking countries. English‑speaking countries are defined as Australia, New Zealand, the United Kingdom, Ireland, the United States, Canada and South Africa. |
People with profound, severe and moderate disability | A person with a profound disability is unable to do, or always needs help with, a core activity task. A person with a severe disability: sometimes needs help with a core activity task, and/or has difficulty understanding or being understood by family or friends, or can communicate more easily using sign language or other non‑spoken forms of communication. A person with a moderate disability needs no help, but has difficulty with a core activity task. |
Personal care | Assistance in undertaking personal tasks (for example, bathing). |
Places | A capacity within an aged care service for the provision of residential care, community care or flexible care in the residential care context to an individual (Aged Care Act 1997 (Cth)); also refers to ‘beds’ (Aged Care (Consequential Provisions) Act 1997 (Cth), s.16). |
Primary carer | In the ABS SDAC, a primary carer is defined as a person who provides the most informal assistance to a person with one or more disabilities, with one or more of the core activities of mobility, self care or communication. |
Respite care | Alternative care arrangements for dependent people living in the community, with the primary purpose of giving a carer or a care recipient a short term break from their usual care arrangement. |
Selected equity groups | Section 11‑3 of the Aged Care Act 1997, specifies the following people as people with special needs: people from Aboriginal and Torres Strait Islander communities; people from culturally and linguistically diverse backgrounds; veterans; people who live in rural or remote areas; people who are financially or socially disadvantaged; people who are homeless or at risk of becoming homeless; care‑leavers; parents separated from their children by forced adoption or removal; and lesbian, gay, bisexual, transgender and intersex people. |
Veterans | Veterans, war widows, widowers and dependants who hold a Repatriation Health Card and are entitled to health services and treatment under the Veterans’ Entitlements Act 1986 (VEA), Safety, Rehabilitation and Compensation Act 1988 (SRCA) or the Military Rehabilitation and Compensation Act 2004 (MRCA). |
References
Aged Care Financing Authority 2021, Ninth Report on the Funding and Financing of the Aged Care Industry − August 2021, https://www.health.gov.au/sites/default/files/documents/2021/08/ninth-report-on-the-funding-and-financing-of-the-aged-care-industry-july-2021.pdf.
ACQSC (Aged Care Quality and Safety Commission) 2021, Annual Report 2020-21, https://www.agedcarequality.gov.au/sites/default/files/media/acqsc-annual-report-2020-21.pdf (accessed 15 November 2021).
—— 2020, Quality Standards, https://www.agedcarequality.gov.au/providers/standards (accessed 4 September 2020).
Aged Care Sector Committee 2020, A Quality Vision for Aged Care, https://www.health.gov.au/resources/publications/a-quality-vision-for-aged-care (accessed 7 September 2020).
ABS 2019, Disability, Ageing and Carers Australia: Summary of Findings 2018, Cat. no. 4430.0, Canberra.
—— 2018a, Population Projections, Australia, 2017, Cat. no. 3222.0, Canberra.
—— 2018b, Life Tables for Aboriginal and Torres Strait Islander Australians, 2015–2017, Cat. no. 3302.0.55.003, Canberra.
AIHW (Australian Institute of Health and Welfare) 2021, Technical notes — National Aged Care Mandatory Quality Indicator Program: 1 January to 31 March 2021, https://gen-agedcaredata.gov.au/www_aihwgen/media/2020-21-Quality-in-aged-care/RACS-QI-technical-notes-Jan-to-Mar-21.pdf (accessed 10 September 2021).
—— 2018, Cause of death patterns and people’s use of aged care: A Pathway in Aged Care analysis of 2012–14 death statistics, Cat. no. AGE 83, AIHW, Canberra.
Department of Health and Aged Care, 2022a, The Australian National Aged Care Classification (AN-ACC) Funding Guide, https://www.health.gov.au/resources/publications/the-australian-national-aged-care-classification-an-acc-funding-guide?language=en (accessed 22 November 2022).
—— 2022b, Aged care data snapshot — 2022, https://www.gen-agedcaredata.gov.au/resources/access-data/2022/october/aged-care-data-snapshot%E2%80%942022 (accessed 20 October 2022).
—— 2021a, 2020 Aged Care Workforce Census Report, Canberra, https://www.health.gov.au/resources/publications/2020-aged-care-workforce-census (accessed 21 October 2022)
—— 2021b, Aged care data snapshot — 2021, https://www.gen-agedcaredata.gov.au/Resources/Access-data/2021/October/Aged-care-data-snapshot%E2%80%942021 (accessed 19 December 2022).
—— 2021c, 2020‑21 Report on the Operation of the Aged Care Act 1997, https://www.health.gov.au/resources/publications/2020-21-report-on-the-operation-of-the-aged-care-act-1997#:~:text=The%20Report%20on%20the%20Operation,Act%20for%20each%20financial%20year. (accessed 20 October 2022).
—— 2021d, National Aged Care Mandatory Quality Indicator Program Manual – 2.0 – Part A https://www.health.gov.au/resources/publications/national-aged-care-mandatory-quality-indicator-program-manual-20-part-a (accessed 22 November 2022).
—— 2017a, 2016 National Aged Care Workforce Census and Survey – The Aged Care Workforce, 2016, Canberra, https://agedcare.health.gov.au/news-and-resources/publications/2016-national-aged-care-workforce-census-and-survey-the-aged-care-workforce-2016 (accessed 20 June 2017).
—— 2017b, National Priority System, https://www.health.gov.au/resources/publications/national-priority-system-for-the-home-care-packages-program (accessed 15 June 2022).
Impact of COVID-19 on data for the Aged care services section
COVID-19 may affect data in this Report in a number of ways. This includes in respect of actual performance (that is, the impact of COVID-19 on service delivery from 2020 to 2022 which is reflected in the data results), and the collection and processing of data (that is, the ability of data providers to undertake data collection and process results for inclusion in the Report).
For the Aged care services section, there has been some impact on the data that is attributable to COVID-19, but this has not affected either the comparability or completeness of any indicators. The data affected relate to the measurement of compliance with aged care quality standards.
Note: An errata was released for section 14 Aged care services above on 14 February 2023.
Errata
The following changes have been made to section 14:
- data table 14A.4 amended to include 2017-18 expenditure data for ‘Residential and Flexible Care Services’ and ‘All Aged Care Services’ for all jurisdictions and per older person aged 50+ (Aboriginal and Torres Strait Islander) and 65+ (Non-Indigenous)
- data table 14A.5 amended to include 2017-18 expenditure data for ‘Other flexible and residential aged care’ and ‘All Aged Care Services’ for all jurisdictions
- Figure 14.1 amended to include 2017-18 data for ‘Residential and Flexible Care Services’ and ‘All Aged Care Services’.
A PDF of Part F Community services can be downloaded from the Part F sector overview page.
12. Social participation in the community